Interview: Dr. Warren M. Levin, MD, Using Neurotransmitter Precursors For Depression, Migraines, And Obesity
October 1, 2010 in Interviews by Tina J. Garcia, with Dr. Warren M. Levin, MD
Five-and-a-half years ago, in November of 2004, I found myself in a desperate and devastating situation. I could barely hold up my head, due to swelling in my brain from a central nervous system infection. My cognitive function was severely impaired, and I could barely walk due to excruciating pain in my legs, ankles and feet.
It was providence that led me to the knowledgeable and compassionate doctor who was able to recognize what no other previous doctor had been able to do. Dr. Warren Levin diagnosed me with Lyme disease and provided the treatment that saved my life!
My heart swells with gratitude for Dr. Levin's response to my situation and for his experience with Lyme disease and other chronic infections. Dr. Levin has for many years engaged in continuing research and study in the pursuit of better treatment outcomes for his patients. He has successfully implemented many innovative methods in his medical practice.
Dr. Levin opened the first Holistic Health Center in New York City in 1974, and his defense of Complementary Medicine for over fourteen years before the Office of Professional Misconduct ended successfully in 1994, leading to the passage of NY State's Alternative Medical Practice Act, and the ignominious defeat of the infamous Victor Herbert, MD, JD, the self-anointed Chief Quackbuster of Mainstream Medicine. Since then, Dr. Levin has been fondly referred to as the Dean of Alternative Medicine on the East Coast.
Tina: Dr. Levin, as always, it's such a pleasure to speak with you. What medical gems of knowledge will you be sharing with us today?
Dr. Levin: Thank you, Tina. It's a pleasure for me, also, since you consulted me early in my short stay in Arizona, and at that time the State's Health Department had seventeen total cases of Lyme disease in Arizona for the entire year of 2003. I found seventeen cases in my first six months in practice, with no patient base to start from, and fortunately, you were an activist. Hopefully, together we have helped to change their focus.
What I'd like to share in this interview is that there is a growing interest within the mainstream medical community in neurotransmitters and the role they play in mental illness. As usual, Complementary physicians have been way ahead of the field, because of our concern for the built-in failure rate of Conventional Psychiatry's approach, and the powerful alternatives available that combine the basic principles of OrthoMolecular Psychiatry, (a term first created by the genius Linus Pauling, PhD as the title for an article in Science Magazine in 1968), and Biochemical Individuality as the title of a book published by another great biochemist of the 20th century - Roger Williams. The most concise expression of those two combined concepts is embodied in a beautiful quotation from a relatively unknown scientist, Emerson Pugh: "If the human brain were simple enough that we could understand it, we would be so simple [minded] that we couldn't understand it!"
Going back in time, the big breakthrough in psychiatry came from Freud coming up with theories about mental illness through his very time-consuming theory of analysis. Even when I was in medical school, his theories were still the major paradigm, but somewhere between then and now behaviorism came into play. Freud said that you cannot change your behavior until you understand why you're behaving that way. The behaviorists said that if you change your behavior intentionally and maintain the change, your brain will convert and act that way by itself. I certainly think that behaviorism is a more efficient method than analysis.
All sorts of methods came about to help people change their attitudes, behaviors and their basic views of life. Still, therapists are constantly trying to make this process easier and more helpful. Then the pharmaceutical industry came into the picture. Again, when I was in medical training, we did not have any tranquilizers or anti-depressants. While I was between my junior and senior years in medical school, I worked in one of the largest insane asylums in the country, Byberry Hospital outside of Philadelphia, Pennsylvania.
My job was to conduct the physical examinations of schizophrenic patients, who were living in horrendous conditions -- worse than being in jail -- and then to follow them to see how they responded to Thorazine, which was the very first anti-psychotic drug. Now the success of that treatment with Thorazine is testified to by the fact that Byberry is basically closed down. What that means is that the people who had been forcibly institutionalized at Byberry, those who were unable to care for themselves and who were risks to themselves and society, were eventually converted into members of that society. They actually became able to live outside of the abominable conditions in the hospital, even though they weren't completely healthy or well. They were not happy or well-adjusted, but some of them were able to hold menial jobs. So, due to this success with the use of Thorazine, the drug-oriented treatment of psychiatric disorders was born.
After that, I think the next thing that came along were called tranquilizers, such as Miltown (Meprobamate). With the use of "downers" and "uppers", the use of psychiatric drugs for socially happy purposes began, with healthy people taking the drugs to feel good and get either high with amphetamines (by prescription only of course), or to zone out with prescribed anti-anxiety drugs. Unfortunately, we have gone on from there.
What I think is now most horrifying is the idea that we are giving children of younger and younger ages psychotropic drugs to make them conform to somebody's standards of acceptable behavior. Ritalin was the first that I am aware of that was used specifically for Attention Deficit Hyperactivity Disorder (ADHD), and it continues to be a mainstay, along with the other class of "uppers" - the Amphetamines. As an example of our continuing ignorance, we still do not understand why the uppers calm down the hyperactive kids, and the downers also work paradoxically to get them "wound up."
It is interesting to note that the pharmacological action of Ritalin is identical to that of cocaine, except that it has a slower onset and is of longer duration. So, with Ritalin, you get the same effect, but it is delayed and is longer-acting. At the same time that we tell kids to stay away from drugs like cocaine, with the other hand, we give them these cocaine-like drugs. I use a different definition of ADHD that I picked up from one of my colleagues, Mary Ann Block, DO. She said it stands for "Another Doctor Handing out Drugs."
Many of the medications that are being used today are from a group of drugs in which they don't really know the mechanism of the action of the drug, the biochemistry isn't certain and exactly where it works in the brain isn't certain, either. However, we give it to people merely because "it works." Although we have no idea of what's going to happen after many years of taking these drugs, they are prescribed anyway. This results in the fact that we are truly a drugged society, and the people who are responsible for bringing this about support each other by making up new diagnostic codes for mental disorders. It appears that as soon as they make one up, they have a drug ready for treatment.
I'll give you an example. PMS has been given a fancy name now -- "Premenstrual Dysphoric Disorder." I laughed when I heard it called pre-menstrual syndrome. Although it is hormonal in nature, it's no longer treated with hormones; it's now treated with psychotropic drugs.
Moving on to depression, one of the really sad things about this whole drug treatment scenario is that people do frequently feel better with the newer drugs (the general class of "reuptake inhibitors"), but unfortunately, that feeling doesn't last. So, they use a little more, which helps again, and then it wears off and they go on to take a higher dose. They eventually run into total resistance in which they don't get any benefit out of it, or they get side effects that are worse than what they were treating. Sometimes, patients cannot afford to pay for the medication, because the insurance companies won't continue to provide insurance coverage. In any event, when people try to stop taking the drugs, they can't stop taking them due to the immense side effects caused by stopping. Thus, stopping the drugs abruptly causes them to crash.
A really unfortunate aspect in dealing with depression and marital relationships is that two of the most important side effects of the class of drugs that is most prescribed for depression now (that is, the SSRI's or selective serotonin reuptake inhibitors) are weight gain and loss of libido. The first SSRI on the market was Prozac and to give it its fair due, it was truly the first medication that depressed patients could take that would, within a matter of days, transform them from deep depression into a functional state.
This transformation is truly amazing, but it doesn't last. So, doses are increased and it works again, but not quite as well. Then patients end up taking more and experience more of the above side effects. If you place those symptoms into the picture of marital UNbliss, it can be devastating to the relationship. There are many couples who have stayed together for years when one of them is really depressed and the other one is the caregiver, but that ends up being too much for many marriages to handle. Adding to the problems, when the patient stops taking the medication, the depression comes back with a vengeance and then the marriage is in a terrible place.
The pharmaceutical industry, however, has continued to churn out antidepressant drugs, based upon the conception that depression is a deficiency of neurotransmitters in the brain. The idea of the way this medicine works sounds clever when you listen to it, but if you think about it for any length of time, you can see that it just cannot possibly be beneficial over the long run. Now, there are exceptions. There may be some people who have been on Prozac for ten years and are functioning, but they are few and far between. Most patients have had terrible difficulties.
The reason for this was pointed out by members of our organization ACAM, the American College for Advancement in Medicine. About seven or eight years ago, there were two doctors who came up with a new approach. One was a medical doctor, who had been working intensively with weight control issues and had developed a way of modifying that behavior using neurotransmitter precursor therapy. His name is Dr. Marty Hinz at this website: www.neuroassist.com.
By the time we heard about this, he had thousands of patient years of experience using these natural substances. He got together with a neurobiochemist, Gottfried Kellerman, PhD, a very bright guy who understood the neurobiochemistry more comprehensively than Dr. Hinz, and the two of them jointly presented their findings. It didn't take long to convince me and many of my colleagues that there was a problem with using selective serotonin re-uptake inhibitors.
The idea that was presented was that the powers that be in psychiatry had decided that the main issue in depression was serotonin deficiency in the brain. Serotonin is one of many neurotransmitters. A neurotransmitter is a substance that transmits a signal, obviously, but from where to where?
The brain is so unbelievably complex that I have on my wall one of the foundational principles of my practice. I again refer to the earlier quote from Emerson Pugh, who wasn't a neurologist or any other kind of doctor, but he came up with a statement that I think is pertinent for the ages when he said, "If the human brain were simple enough that we could understand it, we would be so simple that we couldn't understand it."
I don't think that we will ever truly understand the complexities of our brain, this incredible biochemical computer. Now, I've meditated, I've argued and dissected that statement, and the most important thing to me is this -- what he said is true -- I don't think there is anything that is a misstatement or overstatement in that quotation. I think it says it all, and I question anybody who thinks that it makes sense to put a foreign chemical that has just been discovered in the last fifty years into any brain - most of all not into a child's brain.
Taking into consideration the fact that the human brain has evolved with its environment for the past millenia, it is ludicrous for a doctor with the power to say to a mother, "Well, we have this new drug from ABC Pharmaceutical Company, and they say it's going to help your youngster do well. Now, we don't know how it works yet, but they've tried it out and it's working fine for many of these kids."
That is the most outrageous example of delusional thinking! Hopefully, they won't take me out for making that statement publicly. I think that the psychiatric profession, along with the pharmaceutical industry, has been bought and paid for, and the guys who do it are taking part in a mass psychiatric delusion - they behave as though they really believe that they can "fix" a sick or injured brain with a chemical out of the laboratory. It's just one of the things that I find upsetting about our drug-oriented society.
To understand the relationship between the body and SSRI's, let's take a look at the role of the neurotransmitter, serotonin. Basically, the body has an accelerator and a brake in controlling its various functions. Now, the presence of serotonin, dopamine, norepinephrine and epinephrine-like neurotransmitter substances was discovered within the last seventy-five years. I'm not sure when they decided that it was a deficiency in serotonin that caused depression, but Prozac was the first selective serotonin re-uptake inhibitor used. However, what happens is this -- billions of cells in the brain connect to each other and to other cells, some very far away. By "far away", what I mean is that, if you think about it, the decision to move your right foot forward to walk originates in the brain and finishes in the foot, and the length between these cells can be six or more feet long.
The fact that these actions are accompanied by electrical signals was discovered in the twentieth century. After that was discovered, it was shown through microscopic study that the nerves did not continue all the way to the foot from the brain; they went from the brain to the spinal cord and some of the nerves exited the spinal cord. So, the researchers figured there obviously had to be some connection, so the signal could be transported. As microscopes and technology improved over time, researchers were able to observe that a long nerve fiber from a brain cell goes to the spinal cord and meets another nerve cell in the spinal cord that goes to the foot.
They were then able to observe and measure the electrical signals traveling that route, so it was assumed that the connection between those two nerves represented the resistance to the smooth flow of the electricity. They figured that the nerve kept sending the signal until it built up on the sending side, to the point that it jumped across the gap and stimulated the nerve on the other side, acting very much like the spark plug in an automobile.
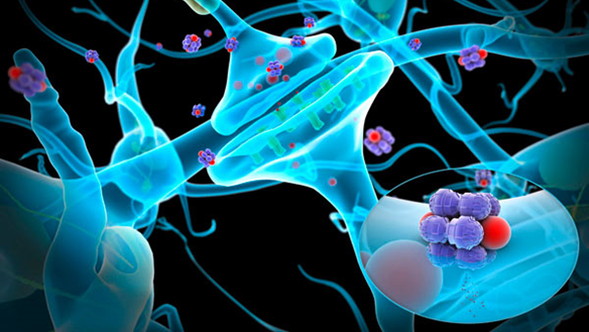
However, it wasn't until late in the twentieth century that it was discovered that it actually wasn't an electrical signal that was transmitted. Researchers found that the electrical signal came down to the end of "the Axon," which is the fiber that carries the signal from a cell away from it, to the synapse, which is where the axon meets a receiving fiber from another nerve cell, "the Dendrite." The synapse is the space between the sending fiber and the receiving fiber, and there is a bulbous bulge at the end of the axon.
They then discovered that the electrical signal triggered the release of chemical substances from the bulb at the end into the synaptic cleft, which is the space between the nerves where they meet. They realized that those substances were transported or being picked up on the other side, and when enough of them were picked up, that's what stimulated the signal to continue. The brain is truly remarkable, and it is interesting to note that the same process occurs in the brains of animals -- mice, cats, dogs, elephants, goats and horses.
One of the major stimulating neurotransmitters that was recognized is serotonin. Researchers wondered how they could get the serotonin to be more effective. Well, neurotransmitters in general are complicated molecules. The body has to manufacture them, and of course the body manufactures them with spare parts that are supplied by the diet. This is an expensive and time consuming process, and therefore, the body does not waste these molecules. So, when they are received into the synapse and they produce the results needed, not all of the supply is used. The body then reabsorbs the neurotransmitter back into the bulb of the axon, so it can be used the next time.
So, quite ingeniously, they developed drugs that block the re-uptake of serotonin, thereby leaving it in the synapse for a longer period of time. This increases the number of receptors that are activated, and therefore, it strengthens the signal. That was a pretty clever idea. And, of course, I'm providing only a basic description of the entire process, but it worked in their experimental situation, so they then tried it on humans. They demonstrated that people really did come out of deep depression. It was almost miraculous and the FDA approved it.
However, no one thought about the issue of whether the problem is really a serotonin deficiency throughout the system. If this is the case, blocking the re-uptake and further lowering the reservoirs will lower the supply more rapidly, because the re-uptake is what keeps them full. Now, the body still manufactures some, but the balance with the proper re-uptake is enough to keep us happy and healthy.
When people have too little serotonin in their reservoirs, and they take these SSRI drugs, their levels are depleted further, and they begin to feel bad while they're on the drugs. The dosage of the drugs then needs to be increased so they feel better again, but the increased dosage lowers the reservoirs even further. Ultimately, this doesn't work, because the reservoirs have run dry. Then when they stop taking the drug, they're in a really bad situation.
This issue was recognized by some of the more objective people working with it and it was referred to as "Prozac poop-out." The pharmaceutical companies did realize that there are other neurotransmitters involved in the process and that one of the problems is the brake and accelerator in our systems.
The spinal cord is a focus of attention for chiropractors and osteopaths, because there is a sympathetic and a parasympathetic nervous system. Each organ responds in its own way to the sympathetic system. And generally speaking, the body responds in the opposite way to the parasympathetic system.
For example, when I was young, I wasn't allowed to go swimming right after I ate, because the function of digestion is the preservation of the body, so that the blood supply is directed towards the digestive system. There is a limited blood supply, so the muscles don't have enough blood supply when we are digesting our food. This causes us to get tired faster, especially while swimming in the water.
The sympathetic system is the fight-fright-flight response. It causes the heart to beat faster, the eyes to dilate, and the blood to flow to the muscles instead of the intestinal tract, so it's not a good idea to eat when you're excited. When it comes to SSRI drugs, what makes it difficult to control is that the serotonin acts as an accelerator in certain areas and in other areas of the brain it acts as a brake. So, you can't just give one drug intending to only stimulate, because in other parts of the body it will act as a suppressant.
The other important issue is that the brain is protected by the blood brain barrier (BBB). There aren't many drugs that can get into the brain, because the brain tries to keep them out with this BBB protection. All of these issues are rolling around in the medication society of today, and the side effects of these medicines present difficulties, as well. More than anything, the pharmaceutical industry has a bonanza, because anyone who starts taking SSRI's and really makes an effort to stick with it, is going to be unable to stop without experiencing some terribly difficult issues.
When people are deeply depressed and then temporarily see the light, they really want to continue seeing the light. So, Dr. Hinz and Dr. Kellerman came up with the idea that, if we give our patients increased amounts of the substances required by the brain to make these neurotransmitters, we could gradually change the brain's balance.
It turns out that this not only works for depression, but in many patients with real serious obesity problems, these neurotransmitter precursors allow them to control appetite, binge eating and all of the other issues, and they lose weight gradually but consistently and feel well while they're doing so. Now that's a pretty amazing thing!
Also, if people who have suffered with migraines for years have the fortitude to try this program, many are able to conquer those terrible headaches, as well. When I began my practice in Virginia, one of my first patients had terrible migraines. I started her on this program and about two weeks later I got a call from a psychiatrist who treated her. She asked me, "What did you give her?" And I answered, "Well, we're using some neurotransmitter precursors." The psychiatrist said, "I've been working with her for years, and since you gave her that stuff, she hasn't had a migraine!"
So, the psychiatrist ended up coming to my office to spend a few days with me and has since attended several of our alternative medicine meetings on using this kind of treatment. I'm not implying that everyone does well; certainly, many depressions are secondary to significant problems that aren't going to be corrected by a drug or a neurotransmitter. However, for the patient with a simple depression not linked to any catastrophic life situation, we have been very fortunate to see many people able to get off these drugs, as difficult as that is. Weaning them off the SSRI's through the use of neurotransmitter precursors enables people to get off the drugs with fewer side effects.
We are such complex organisms that it's foolish to make believe that we understand the body. When I demonstrate this to people, I explain it using a slide show and people can see what happens at the synapse. I ask "What do you think happens to the reservoirs?" And they really understand it. So, I tell them that what we really need to do is to refill the reservoirs. I do not want them to try going off the medication all at once; I want them to stay on the medication and refill the reservoirs from
behind, as well.
Also, there are so many other situations that can contribute to the depression syndrome, and especially with longtime depression, people tend to eat poorly. They don't take care of themselves and they don't exercise, so the body is not contributing to their well being either. We encourage them to exercise, eat the right food and not eat the wrong food. We also measure their vitamin and mineral levels and a number of other substances in their blood. We correct the deficiencies and address the toxins, and they start realizing that they have to take care of the body that's housing this machine.
Once they start getting better, they are eager to stop the medicine. Sometimes we need to kind of sit on them a bit and tell them that they can't just stop taking the medicine all at once. We are feeling our way along, but I have very few people who have continued the program who have not been able to get off the drugs. I've also had a lot of people who start the program, but are too enmeshed in their misery to complete it.
The biggest problem with the protocol in comparison to taking medications like Prozac, Paxil, Zoloft, Cymbalta, Lexapro and now there's Pristique, is that the prescription drugs require only one or two pills a day, but it takes well over twenty pills a day to reach and maintain the repletion of the reservoirs. There are also variations in the balance of the serotonin and the other side, the dopamine/norepinephrine, so that some psychiatrists are better than others with their intuition or understanding of which drugs will work better for each particular person.
When patients' reservoirs are refilled, they can taper off these medicines and they do not hit the wall. We also need to correct their deficiencies and see if they have any toxins. We also look for allergies, because allergies can cause depression. This is especially true about food and drink allergies. So, when you take away the addiction, it speeds up the healing process.
Infections can also cause depression, and here we come to something you know about, knock on wood, Lyme disease. There was a Dr. Paul Fink, who was the President of the American Psychiatric Association some years ago. He said that anytime someone previously healthy suddenly shows up with any kind of psychiatric diagnosis, you should always consider the possibility that it was triggered by Lyme disease. I don't think a lot of psychiatrists think about that possibility. Coincidentally, by six degrees of separation, my brother is best friends with Dr. Fink's brother.
In my opinion, this is another example of how a holistic, complementary, integrative and functional approach works best. You just can't simply treat someone with a pill for their depression. You must look for their allergies, infections and analyze their diet nutrient deficiencies. When you get these things straightened out, they feel better.
One of the sad things is that these two doctors, Dr. Hinz and Dr. Kellerman didn't last together very long. One was a physician/clinician and the other was a neurobiochemist. Dr. Kellerman began looking at all the other neurotransmitters, and when they gave their lecture about eight years ago and they said something like 183 neurotransmitters had been identified, Dr. Kellerman wanted to address all of them.
What Dr. Hinz identified, because he kept incredibly comprehensive records on everyone he treated, was that even though some of these other neurotransmitters might be out of balance, if you straightened out the push and the pull of serotonin on one side and the dopamine on the other side, the other untreated neurotransmitters would fall in line as well.
Dopamine breaks down into norepinephrine (NorAdrenalin being the trade name). Norepinephrine is then broken down into epinephrine (Adrenalin) and epinephrine is the fight-fright-flight response of the sympathetic nervous system, which comes from the adrenal glands. However, when we're experimenting with people, we're experimenting with people's brains. They had to demonstrate that the adrenal epinephrine did not act as the same neurotransmitter in the brain and you can't give neurotransmitters orally or by injection, because they don't cross the blood brain barrier. That is why we need to give the precursor molecules, so that the body will manufacture them naturally and fill the reservoirs.
So, I have had to choose sides in yet another controversy. I have been working with Dr. Hinz, who has a company called Neuro Research, and Dr. Kellerman has a company called NeuroScience. His company works on a lot of things besides depression. The thing that Dr. Kellerman does first is test the neurotransmitters, and this is how he determines what needs to be treated.
Now, Dr. Hinz refuses to do that, because he has done a great deal of research and found that what is in the blood or the urine is not in the brain, until you have people on these high doses for some time. I think that is scientifically established with peer-reviewed literature, most of which was contributed by Dr. Hinz. I think that was what led to the demise of the relationship, because Dr. Kellerman analyzes many different neurotransmitter combinations.
However, the evidence does show that focusing on those two major neurotransmitters, serotonin and dopamine, and keeping their levels steady, allows everything else to fall into place. This results in a lot less testing and complicated drugs and supplements. After people have been on a steady dose of neurotransmitter precursors for some time, the levels in the blood and urine begin to reflect what is happening in the brain. This is a very complicated interpretation, so I send the labs in for helpful suggestions for changes in the therapy. Every once in a while, we get some scrambled test results, but over the long run, the results have been very successful. I think this is so much better than what's out there in mainstream medicine. However, that's the system that prevails. They're psychiatrists. Why should they worry about these issues? They let somebody else worry about them. They don't do the workups or send the patients out for workups; they just treat them with drugs.
Tina: This is really important work. Thank you so much for pursuing this on behalf of patients.
Dr. Levin: I'm honored to be doing it. I feel blessed to have been introduced to it, and to have listened to it, believed it and tried it. It is really important and quite effective in the right situations with the right patients.
I've also been involved with an alternative approach to diagnosing and treating thyroid dysfunction. The Wilson's Thyroid Syndrome organization holds an annual meeting and this year it will be held in Utah in October. For the second time, I will be lecturing. I'm hoping that Dr. Hinz will be included in that program, too. I'm trying to get the word out for him on this topic, as he has really performed a great service to mankind through his research and findings.
Tina: How would neurotransmitter precursor therapy work in patients with Lyme disease?
Dr. Levin: In patients with Lyme disease who are taking antidepressant drugs, the drug adds an additional stress that they're not even aware of. I will start them on this program, so they can get off the drugs. Some people say Lyme patients are chronically ill because they're depressed, but I don't think that's the likely scenario. Actually, many chronically-ill patients are depressed because they're chronically ill. In some instances, when we get under control whatever the chronic problem is, they are able to come out of it without the drugs and without the alternative program.
Tina: It appears to me that if a person has a chronic infection that affects the nervous system, such as Lyme disease, and it has thrown the system out of whack, that it may be a horrendous situation to add drugs into the mix, which can throw it out of whack even more. Would this also apply to Parkinson's?
Dr. Levin: This is a very important topic for patients to understand, especially those with any chronic infection. Parkinson's is a pretty radical degree of dopamine dysfunction. Mainstream docs use dopamine agonists in the treatment of Parkinson's, but it seems that the nerves that produce dopamine in these areas are damaged somehow. Yet, some people are able to use these precursors and have the symptoms improve. I've had a couple of good results, but I've seen more failures with Parkinson's than with any of the others.
Tina: What final words of wisdom would you like to offer, Dr. Levin?
Dr. Levin: Eat the right food, exercise regularly, and take supplements to make up for the lousy food supply that we've created in this country. Absolutely do not eat any genetically modified foods, such as soy, corn and cottonseed. Eat organic. Unless it's marked organic, don't eat any soy or corn. More than 80 percent of the soy in this country is genetically modified and a very high percentage of corn and its derivatives are modified, also. We have no business messing with the gene pool. I also suggest doing something that will bring you psycho-spiritual equilibrium.
It was providence that led me to the knowledgeable and compassionate doctor who was able to recognize what no other previous doctor had been able to do. Dr. Warren Levin diagnosed me with Lyme disease and provided the treatment that saved my life!
My heart swells with gratitude for Dr. Levin's response to my situation and for his experience with Lyme disease and other chronic infections. Dr. Levin has for many years engaged in continuing research and study in the pursuit of better treatment outcomes for his patients. He has successfully implemented many innovative methods in his medical practice.
Dr. Levin opened the first Holistic Health Center in New York City in 1974, and his defense of Complementary Medicine for over fourteen years before the Office of Professional Misconduct ended successfully in 1994, leading to the passage of NY State's Alternative Medical Practice Act, and the ignominious defeat of the infamous Victor Herbert, MD, JD, the self-anointed Chief Quackbuster of Mainstream Medicine. Since then, Dr. Levin has been fondly referred to as the Dean of Alternative Medicine on the East Coast.
Tina: Dr. Levin, as always, it's such a pleasure to speak with you. What medical gems of knowledge will you be sharing with us today?
Dr. Levin: Thank you, Tina. It's a pleasure for me, also, since you consulted me early in my short stay in Arizona, and at that time the State's Health Department had seventeen total cases of Lyme disease in Arizona for the entire year of 2003. I found seventeen cases in my first six months in practice, with no patient base to start from, and fortunately, you were an activist. Hopefully, together we have helped to change their focus.
What I'd like to share in this interview is that there is a growing interest within the mainstream medical community in neurotransmitters and the role they play in mental illness. As usual, Complementary physicians have been way ahead of the field, because of our concern for the built-in failure rate of Conventional Psychiatry's approach, and the powerful alternatives available that combine the basic principles of OrthoMolecular Psychiatry, (a term first created by the genius Linus Pauling, PhD as the title for an article in Science Magazine in 1968), and Biochemical Individuality as the title of a book published by another great biochemist of the 20th century - Roger Williams. The most concise expression of those two combined concepts is embodied in a beautiful quotation from a relatively unknown scientist, Emerson Pugh: "If the human brain were simple enough that we could understand it, we would be so simple [minded] that we couldn't understand it!"
Going back in time, the big breakthrough in psychiatry came from Freud coming up with theories about mental illness through his very time-consuming theory of analysis. Even when I was in medical school, his theories were still the major paradigm, but somewhere between then and now behaviorism came into play. Freud said that you cannot change your behavior until you understand why you're behaving that way. The behaviorists said that if you change your behavior intentionally and maintain the change, your brain will convert and act that way by itself. I certainly think that behaviorism is a more efficient method than analysis.
All sorts of methods came about to help people change their attitudes, behaviors and their basic views of life. Still, therapists are constantly trying to make this process easier and more helpful. Then the pharmaceutical industry came into the picture. Again, when I was in medical training, we did not have any tranquilizers or anti-depressants. While I was between my junior and senior years in medical school, I worked in one of the largest insane asylums in the country, Byberry Hospital outside of Philadelphia, Pennsylvania.
My job was to conduct the physical examinations of schizophrenic patients, who were living in horrendous conditions -- worse than being in jail -- and then to follow them to see how they responded to Thorazine, which was the very first anti-psychotic drug. Now the success of that treatment with Thorazine is testified to by the fact that Byberry is basically closed down. What that means is that the people who had been forcibly institutionalized at Byberry, those who were unable to care for themselves and who were risks to themselves and society, were eventually converted into members of that society. They actually became able to live outside of the abominable conditions in the hospital, even though they weren't completely healthy or well. They were not happy or well-adjusted, but some of them were able to hold menial jobs. So, due to this success with the use of Thorazine, the drug-oriented treatment of psychiatric disorders was born.
After that, I think the next thing that came along were called tranquilizers, such as Miltown (Meprobamate). With the use of "downers" and "uppers", the use of psychiatric drugs for socially happy purposes began, with healthy people taking the drugs to feel good and get either high with amphetamines (by prescription only of course), or to zone out with prescribed anti-anxiety drugs. Unfortunately, we have gone on from there.
What I think is now most horrifying is the idea that we are giving children of younger and younger ages psychotropic drugs to make them conform to somebody's standards of acceptable behavior. Ritalin was the first that I am aware of that was used specifically for Attention Deficit Hyperactivity Disorder (ADHD), and it continues to be a mainstay, along with the other class of "uppers" - the Amphetamines. As an example of our continuing ignorance, we still do not understand why the uppers calm down the hyperactive kids, and the downers also work paradoxically to get them "wound up."
It is interesting to note that the pharmacological action of Ritalin is identical to that of cocaine, except that it has a slower onset and is of longer duration. So, with Ritalin, you get the same effect, but it is delayed and is longer-acting. At the same time that we tell kids to stay away from drugs like cocaine, with the other hand, we give them these cocaine-like drugs. I use a different definition of ADHD that I picked up from one of my colleagues, Mary Ann Block, DO. She said it stands for "Another Doctor Handing out Drugs."
Many of the medications that are being used today are from a group of drugs in which they don't really know the mechanism of the action of the drug, the biochemistry isn't certain and exactly where it works in the brain isn't certain, either. However, we give it to people merely because "it works." Although we have no idea of what's going to happen after many years of taking these drugs, they are prescribed anyway. This results in the fact that we are truly a drugged society, and the people who are responsible for bringing this about support each other by making up new diagnostic codes for mental disorders. It appears that as soon as they make one up, they have a drug ready for treatment.
I'll give you an example. PMS has been given a fancy name now -- "Premenstrual Dysphoric Disorder." I laughed when I heard it called pre-menstrual syndrome. Although it is hormonal in nature, it's no longer treated with hormones; it's now treated with psychotropic drugs.
Moving on to depression, one of the really sad things about this whole drug treatment scenario is that people do frequently feel better with the newer drugs (the general class of "reuptake inhibitors"), but unfortunately, that feeling doesn't last. So, they use a little more, which helps again, and then it wears off and they go on to take a higher dose. They eventually run into total resistance in which they don't get any benefit out of it, or they get side effects that are worse than what they were treating. Sometimes, patients cannot afford to pay for the medication, because the insurance companies won't continue to provide insurance coverage. In any event, when people try to stop taking the drugs, they can't stop taking them due to the immense side effects caused by stopping. Thus, stopping the drugs abruptly causes them to crash.
A really unfortunate aspect in dealing with depression and marital relationships is that two of the most important side effects of the class of drugs that is most prescribed for depression now (that is, the SSRI's or selective serotonin reuptake inhibitors) are weight gain and loss of libido. The first SSRI on the market was Prozac and to give it its fair due, it was truly the first medication that depressed patients could take that would, within a matter of days, transform them from deep depression into a functional state.
This transformation is truly amazing, but it doesn't last. So, doses are increased and it works again, but not quite as well. Then patients end up taking more and experience more of the above side effects. If you place those symptoms into the picture of marital UNbliss, it can be devastating to the relationship. There are many couples who have stayed together for years when one of them is really depressed and the other one is the caregiver, but that ends up being too much for many marriages to handle. Adding to the problems, when the patient stops taking the medication, the depression comes back with a vengeance and then the marriage is in a terrible place.
The pharmaceutical industry, however, has continued to churn out antidepressant drugs, based upon the conception that depression is a deficiency of neurotransmitters in the brain. The idea of the way this medicine works sounds clever when you listen to it, but if you think about it for any length of time, you can see that it just cannot possibly be beneficial over the long run. Now, there are exceptions. There may be some people who have been on Prozac for ten years and are functioning, but they are few and far between. Most patients have had terrible difficulties.
The reason for this was pointed out by members of our organization ACAM, the American College for Advancement in Medicine. About seven or eight years ago, there were two doctors who came up with a new approach. One was a medical doctor, who had been working intensively with weight control issues and had developed a way of modifying that behavior using neurotransmitter precursor therapy. His name is Dr. Marty Hinz at this website: www.neuroassist.com.
By the time we heard about this, he had thousands of patient years of experience using these natural substances. He got together with a neurobiochemist, Gottfried Kellerman, PhD, a very bright guy who understood the neurobiochemistry more comprehensively than Dr. Hinz, and the two of them jointly presented their findings. It didn't take long to convince me and many of my colleagues that there was a problem with using selective serotonin re-uptake inhibitors.
The idea that was presented was that the powers that be in psychiatry had decided that the main issue in depression was serotonin deficiency in the brain. Serotonin is one of many neurotransmitters. A neurotransmitter is a substance that transmits a signal, obviously, but from where to where?
The brain is so unbelievably complex that I have on my wall one of the foundational principles of my practice. I again refer to the earlier quote from Emerson Pugh, who wasn't a neurologist or any other kind of doctor, but he came up with a statement that I think is pertinent for the ages when he said, "If the human brain were simple enough that we could understand it, we would be so simple that we couldn't understand it."
I don't think that we will ever truly understand the complexities of our brain, this incredible biochemical computer. Now, I've meditated, I've argued and dissected that statement, and the most important thing to me is this -- what he said is true -- I don't think there is anything that is a misstatement or overstatement in that quotation. I think it says it all, and I question anybody who thinks that it makes sense to put a foreign chemical that has just been discovered in the last fifty years into any brain - most of all not into a child's brain.
Taking into consideration the fact that the human brain has evolved with its environment for the past millenia, it is ludicrous for a doctor with the power to say to a mother, "Well, we have this new drug from ABC Pharmaceutical Company, and they say it's going to help your youngster do well. Now, we don't know how it works yet, but they've tried it out and it's working fine for many of these kids."
That is the most outrageous example of delusional thinking! Hopefully, they won't take me out for making that statement publicly. I think that the psychiatric profession, along with the pharmaceutical industry, has been bought and paid for, and the guys who do it are taking part in a mass psychiatric delusion - they behave as though they really believe that they can "fix" a sick or injured brain with a chemical out of the laboratory. It's just one of the things that I find upsetting about our drug-oriented society.
To understand the relationship between the body and SSRI's, let's take a look at the role of the neurotransmitter, serotonin. Basically, the body has an accelerator and a brake in controlling its various functions. Now, the presence of serotonin, dopamine, norepinephrine and epinephrine-like neurotransmitter substances was discovered within the last seventy-five years. I'm not sure when they decided that it was a deficiency in serotonin that caused depression, but Prozac was the first selective serotonin re-uptake inhibitor used. However, what happens is this -- billions of cells in the brain connect to each other and to other cells, some very far away. By "far away", what I mean is that, if you think about it, the decision to move your right foot forward to walk originates in the brain and finishes in the foot, and the length between these cells can be six or more feet long.
The fact that these actions are accompanied by electrical signals was discovered in the twentieth century. After that was discovered, it was shown through microscopic study that the nerves did not continue all the way to the foot from the brain; they went from the brain to the spinal cord and some of the nerves exited the spinal cord. So, the researchers figured there obviously had to be some connection, so the signal could be transported. As microscopes and technology improved over time, researchers were able to observe that a long nerve fiber from a brain cell goes to the spinal cord and meets another nerve cell in the spinal cord that goes to the foot.
They were then able to observe and measure the electrical signals traveling that route, so it was assumed that the connection between those two nerves represented the resistance to the smooth flow of the electricity. They figured that the nerve kept sending the signal until it built up on the sending side, to the point that it jumped across the gap and stimulated the nerve on the other side, acting very much like the spark plug in an automobile.
However, it wasn't until late in the twentieth century that it was discovered that it actually wasn't an electrical signal that was transmitted. Researchers found that the electrical signal came down to the end of "the Axon," which is the fiber that carries the signal from a cell away from it, to the synapse, which is where the axon meets a receiving fiber from another nerve cell, "the Dendrite." The synapse is the space between the sending fiber and the receiving fiber, and there is a bulbous bulge at the end of the axon.
They then discovered that the electrical signal triggered the release of chemical substances from the bulb at the end into the synaptic cleft, which is the space between the nerves where they meet. They realized that those substances were transported or being picked up on the other side, and when enough of them were picked up, that's what stimulated the signal to continue. The brain is truly remarkable, and it is interesting to note that the same process occurs in the brains of animals -- mice, cats, dogs, elephants, goats and horses.
One of the major stimulating neurotransmitters that was recognized is serotonin. Researchers wondered how they could get the serotonin to be more effective. Well, neurotransmitters in general are complicated molecules. The body has to manufacture them, and of course the body manufactures them with spare parts that are supplied by the diet. This is an expensive and time consuming process, and therefore, the body does not waste these molecules. So, when they are received into the synapse and they produce the results needed, not all of the supply is used. The body then reabsorbs the neurotransmitter back into the bulb of the axon, so it can be used the next time.
So, quite ingeniously, they developed drugs that block the re-uptake of serotonin, thereby leaving it in the synapse for a longer period of time. This increases the number of receptors that are activated, and therefore, it strengthens the signal. That was a pretty clever idea. And, of course, I'm providing only a basic description of the entire process, but it worked in their experimental situation, so they then tried it on humans. They demonstrated that people really did come out of deep depression. It was almost miraculous and the FDA approved it.
However, no one thought about the issue of whether the problem is really a serotonin deficiency throughout the system. If this is the case, blocking the re-uptake and further lowering the reservoirs will lower the supply more rapidly, because the re-uptake is what keeps them full. Now, the body still manufactures some, but the balance with the proper re-uptake is enough to keep us happy and healthy.
When people have too little serotonin in their reservoirs, and they take these SSRI drugs, their levels are depleted further, and they begin to feel bad while they're on the drugs. The dosage of the drugs then needs to be increased so they feel better again, but the increased dosage lowers the reservoirs even further. Ultimately, this doesn't work, because the reservoirs have run dry. Then when they stop taking the drug, they're in a really bad situation.
This issue was recognized by some of the more objective people working with it and it was referred to as "Prozac poop-out." The pharmaceutical companies did realize that there are other neurotransmitters involved in the process and that one of the problems is the brake and accelerator in our systems.
The spinal cord is a focus of attention for chiropractors and osteopaths, because there is a sympathetic and a parasympathetic nervous system. Each organ responds in its own way to the sympathetic system. And generally speaking, the body responds in the opposite way to the parasympathetic system.
For example, when I was young, I wasn't allowed to go swimming right after I ate, because the function of digestion is the preservation of the body, so that the blood supply is directed towards the digestive system. There is a limited blood supply, so the muscles don't have enough blood supply when we are digesting our food. This causes us to get tired faster, especially while swimming in the water.
The sympathetic system is the fight-fright-flight response. It causes the heart to beat faster, the eyes to dilate, and the blood to flow to the muscles instead of the intestinal tract, so it's not a good idea to eat when you're excited. When it comes to SSRI drugs, what makes it difficult to control is that the serotonin acts as an accelerator in certain areas and in other areas of the brain it acts as a brake. So, you can't just give one drug intending to only stimulate, because in other parts of the body it will act as a suppressant.
The other important issue is that the brain is protected by the blood brain barrier (BBB). There aren't many drugs that can get into the brain, because the brain tries to keep them out with this BBB protection. All of these issues are rolling around in the medication society of today, and the side effects of these medicines present difficulties, as well. More than anything, the pharmaceutical industry has a bonanza, because anyone who starts taking SSRI's and really makes an effort to stick with it, is going to be unable to stop without experiencing some terribly difficult issues.
When people are deeply depressed and then temporarily see the light, they really want to continue seeing the light. So, Dr. Hinz and Dr. Kellerman came up with the idea that, if we give our patients increased amounts of the substances required by the brain to make these neurotransmitters, we could gradually change the brain's balance.
It turns out that this not only works for depression, but in many patients with real serious obesity problems, these neurotransmitter precursors allow them to control appetite, binge eating and all of the other issues, and they lose weight gradually but consistently and feel well while they're doing so. Now that's a pretty amazing thing!
Also, if people who have suffered with migraines for years have the fortitude to try this program, many are able to conquer those terrible headaches, as well. When I began my practice in Virginia, one of my first patients had terrible migraines. I started her on this program and about two weeks later I got a call from a psychiatrist who treated her. She asked me, "What did you give her?" And I answered, "Well, we're using some neurotransmitter precursors." The psychiatrist said, "I've been working with her for years, and since you gave her that stuff, she hasn't had a migraine!"
So, the psychiatrist ended up coming to my office to spend a few days with me and has since attended several of our alternative medicine meetings on using this kind of treatment. I'm not implying that everyone does well; certainly, many depressions are secondary to significant problems that aren't going to be corrected by a drug or a neurotransmitter. However, for the patient with a simple depression not linked to any catastrophic life situation, we have been very fortunate to see many people able to get off these drugs, as difficult as that is. Weaning them off the SSRI's through the use of neurotransmitter precursors enables people to get off the drugs with fewer side effects.
We are such complex organisms that it's foolish to make believe that we understand the body. When I demonstrate this to people, I explain it using a slide show and people can see what happens at the synapse. I ask "What do you think happens to the reservoirs?" And they really understand it. So, I tell them that what we really need to do is to refill the reservoirs. I do not want them to try going off the medication all at once; I want them to stay on the medication and refill the reservoirs from
behind, as well.
Also, there are so many other situations that can contribute to the depression syndrome, and especially with longtime depression, people tend to eat poorly. They don't take care of themselves and they don't exercise, so the body is not contributing to their well being either. We encourage them to exercise, eat the right food and not eat the wrong food. We also measure their vitamin and mineral levels and a number of other substances in their blood. We correct the deficiencies and address the toxins, and they start realizing that they have to take care of the body that's housing this machine.
Once they start getting better, they are eager to stop the medicine. Sometimes we need to kind of sit on them a bit and tell them that they can't just stop taking the medicine all at once. We are feeling our way along, but I have very few people who have continued the program who have not been able to get off the drugs. I've also had a lot of people who start the program, but are too enmeshed in their misery to complete it.
The biggest problem with the protocol in comparison to taking medications like Prozac, Paxil, Zoloft, Cymbalta, Lexapro and now there's Pristique, is that the prescription drugs require only one or two pills a day, but it takes well over twenty pills a day to reach and maintain the repletion of the reservoirs. There are also variations in the balance of the serotonin and the other side, the dopamine/norepinephrine, so that some psychiatrists are better than others with their intuition or understanding of which drugs will work better for each particular person.
When patients' reservoirs are refilled, they can taper off these medicines and they do not hit the wall. We also need to correct their deficiencies and see if they have any toxins. We also look for allergies, because allergies can cause depression. This is especially true about food and drink allergies. So, when you take away the addiction, it speeds up the healing process.
Infections can also cause depression, and here we come to something you know about, knock on wood, Lyme disease. There was a Dr. Paul Fink, who was the President of the American Psychiatric Association some years ago. He said that anytime someone previously healthy suddenly shows up with any kind of psychiatric diagnosis, you should always consider the possibility that it was triggered by Lyme disease. I don't think a lot of psychiatrists think about that possibility. Coincidentally, by six degrees of separation, my brother is best friends with Dr. Fink's brother.
In my opinion, this is another example of how a holistic, complementary, integrative and functional approach works best. You just can't simply treat someone with a pill for their depression. You must look for their allergies, infections and analyze their diet nutrient deficiencies. When you get these things straightened out, they feel better.
One of the sad things is that these two doctors, Dr. Hinz and Dr. Kellerman didn't last together very long. One was a physician/clinician and the other was a neurobiochemist. Dr. Kellerman began looking at all the other neurotransmitters, and when they gave their lecture about eight years ago and they said something like 183 neurotransmitters had been identified, Dr. Kellerman wanted to address all of them.
What Dr. Hinz identified, because he kept incredibly comprehensive records on everyone he treated, was that even though some of these other neurotransmitters might be out of balance, if you straightened out the push and the pull of serotonin on one side and the dopamine on the other side, the other untreated neurotransmitters would fall in line as well.
Dopamine breaks down into norepinephrine (NorAdrenalin being the trade name). Norepinephrine is then broken down into epinephrine (Adrenalin) and epinephrine is the fight-fright-flight response of the sympathetic nervous system, which comes from the adrenal glands. However, when we're experimenting with people, we're experimenting with people's brains. They had to demonstrate that the adrenal epinephrine did not act as the same neurotransmitter in the brain and you can't give neurotransmitters orally or by injection, because they don't cross the blood brain barrier. That is why we need to give the precursor molecules, so that the body will manufacture them naturally and fill the reservoirs.
So, I have had to choose sides in yet another controversy. I have been working with Dr. Hinz, who has a company called Neuro Research, and Dr. Kellerman has a company called NeuroScience. His company works on a lot of things besides depression. The thing that Dr. Kellerman does first is test the neurotransmitters, and this is how he determines what needs to be treated.
Now, Dr. Hinz refuses to do that, because he has done a great deal of research and found that what is in the blood or the urine is not in the brain, until you have people on these high doses for some time. I think that is scientifically established with peer-reviewed literature, most of which was contributed by Dr. Hinz. I think that was what led to the demise of the relationship, because Dr. Kellerman analyzes many different neurotransmitter combinations.
However, the evidence does show that focusing on those two major neurotransmitters, serotonin and dopamine, and keeping their levels steady, allows everything else to fall into place. This results in a lot less testing and complicated drugs and supplements. After people have been on a steady dose of neurotransmitter precursors for some time, the levels in the blood and urine begin to reflect what is happening in the brain. This is a very complicated interpretation, so I send the labs in for helpful suggestions for changes in the therapy. Every once in a while, we get some scrambled test results, but over the long run, the results have been very successful. I think this is so much better than what's out there in mainstream medicine. However, that's the system that prevails. They're psychiatrists. Why should they worry about these issues? They let somebody else worry about them. They don't do the workups or send the patients out for workups; they just treat them with drugs.
Tina: This is really important work. Thank you so much for pursuing this on behalf of patients.
Dr. Levin: I'm honored to be doing it. I feel blessed to have been introduced to it, and to have listened to it, believed it and tried it. It is really important and quite effective in the right situations with the right patients.
I've also been involved with an alternative approach to diagnosing and treating thyroid dysfunction. The Wilson's Thyroid Syndrome organization holds an annual meeting and this year it will be held in Utah in October. For the second time, I will be lecturing. I'm hoping that Dr. Hinz will be included in that program, too. I'm trying to get the word out for him on this topic, as he has really performed a great service to mankind through his research and findings.
Tina: How would neurotransmitter precursor therapy work in patients with Lyme disease?
Dr. Levin: In patients with Lyme disease who are taking antidepressant drugs, the drug adds an additional stress that they're not even aware of. I will start them on this program, so they can get off the drugs. Some people say Lyme patients are chronically ill because they're depressed, but I don't think that's the likely scenario. Actually, many chronically-ill patients are depressed because they're chronically ill. In some instances, when we get under control whatever the chronic problem is, they are able to come out of it without the drugs and without the alternative program.
Tina: It appears to me that if a person has a chronic infection that affects the nervous system, such as Lyme disease, and it has thrown the system out of whack, that it may be a horrendous situation to add drugs into the mix, which can throw it out of whack even more. Would this also apply to Parkinson's?
Dr. Levin: This is a very important topic for patients to understand, especially those with any chronic infection. Parkinson's is a pretty radical degree of dopamine dysfunction. Mainstream docs use dopamine agonists in the treatment of Parkinson's, but it seems that the nerves that produce dopamine in these areas are damaged somehow. Yet, some people are able to use these precursors and have the symptoms improve. I've had a couple of good results, but I've seen more failures with Parkinson's than with any of the others.
Tina: What final words of wisdom would you like to offer, Dr. Levin?
Dr. Levin: Eat the right food, exercise regularly, and take supplements to make up for the lousy food supply that we've created in this country. Absolutely do not eat any genetically modified foods, such as soy, corn and cottonseed. Eat organic. Unless it's marked organic, don't eat any soy or corn. More than 80 percent of the soy in this country is genetically modified and a very high percentage of corn and its derivatives are modified, also. We have no business messing with the gene pool. I also suggest doing something that will bring you psycho-spiritual equilibrium.
About the author

Dr. Levin has a private practice in Vienna, Virginia. Visit his website at http://www.warrenmlevinmd.org
About the author

Tina Juliette Garcia is a freelance writer, Lyme disease patient and advocate who founded Lyme Education Awareness Program, L.E.A.P. Arizona, a non-profit that provides education about Lyme disease and co-infections. Visit her website at www.leaparizona.com.
Tina is currently focusing her service to the chronic illness patient community through Massage Therapy, Aromatherapy and Life Coaching. Tina is offering COMPLIMENTARY LIFE COACHING sessions to introduce patients to a new perspective on wellness through the MIND-BODY-SPIRIT CONNECTION.
Tina is currently focusing her service to the chronic illness patient community through Massage Therapy, Aromatherapy and Life Coaching. Tina is offering COMPLIMENTARY LIFE COACHING sessions to introduce patients to a new perspective on wellness through the MIND-BODY-SPIRIT CONNECTION.
latest posts

tags
Cowden Protocol month 1

23andMe genetic Testing
Disclaimer: The information on this website is not a substitute for professional medical advice.
Always consult with your treating physician before altering any treatment protocol.
Always consult with your treating physician before altering any treatment protocol.
