Candida Related Complex: A Complicating Factor In Lyme Disease
May 1, 2008 in Science/Research by Scott Forsgren
For many people struggling with chronic Lyme disease, symptoms such as headaches, inability to think clearly, mood swings, muscle aches, joint pain, poor memory, depression, sinus congestion, allergies, chemical sensitivities, digestive disturbances, fatigue, anxiety, and skin rashes are not uncommon. What may not be readily apparent, however, is that these same symptoms, and others, are attributable to a common yeast called Candida (can'-di-duh), which results in what has been termed "Candida Related Complex". A failure to understand and address this issue may result in a less than optimal overall Lyme disease treatment outcome.
Warren M. Levin, MD, PLLC blends conventional and alternative medical philosophies in his private practice in Vienna, VA. Dr. Levin has found Candida Related Complex (CRC) to be a significant factor in the presentation of many chronic conditions. Dr. Levin identifies CRC as a common iatrogenic complication in the majority of people with Lyme disease and believes that it must be adequately addressed in order to return one to an ideal state of health and wellness.
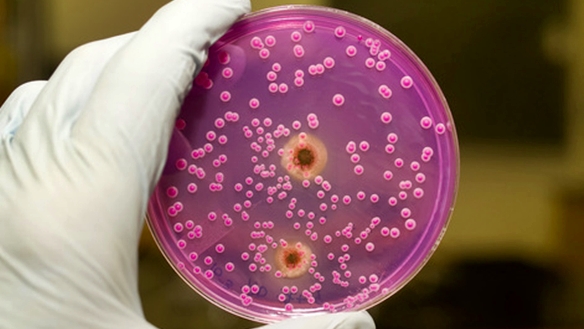
Of the family of yeasts known as Candida, Candida albicans is the most common, though there are numerous species that may result in clinical symptoms. Symptoms of Candida can affect every bodily system and are often incapacitating.
The majority of practitioners in mainstream medicine today still do not recognize the importance of the presence of Candida on overall health. They often suggest that Candida is only an issue in patients that are severely immunocompromised, such as patients with HIV, cancer, or patients that have undergone chemotherapy or radiation. This perspective is quite limited and misses the majority of patients whose health is in fact impacted by Candida.
Candida Related Complex has been called the "Yeast Syndrome", the "Yeast Connection", and Thrush, among other terms. It has also been called "imaginary", "nonsense", "fraud", and "charlatanism" by those that do not understand its implications and prevalence.
Not only does Dr. Levin believe that CRC is real, often overlooked and generally under-treated, but he has found that many people with a diagnosis of Lyme disease are experiencing symptoms that are partially, or entirely, attributable to Candida Related Complex, not to Lyme disease itself. Since the mid 20th century, five major changes in Western societies have created the perfect storm for establishment of Candida Related Complex:
1. The tremendous increase in refined and processed foods, especially sugars and chemical additives.
2. The introduction - and overuse - of antibiotics.
3. The introduction - and overuse - of cortisone and its natural and artificial derivatives.
4. The introduction and widespread use of Birth Control Pills, which are supposed to be "estrogen and progesterone" combinations, but are actually artificial, synthesized foreign molecules that are very successful in preventing pregnancy. Unfortunately, they also interfere with normal hormonal balances, and produce changes in the vaginal tissues that predispose women to Candida infection.
5. The introduction- and overuse - of drugs that suppress stomach acid production, thus depriving the users of the normal killing of foreign organisms that are ingested with food (such as Candida) and also preventing the proper digestion of protein which over time leads to malnutrition, even with healthy diets.
Dr. Levin believes that CRC is a complex problem which plays a role in multiple chronic and degenerative disease syndromes. CRC is more than just a yeast infection. In fact, most often, CRC exists without the presence of an obvious yeast infection. The belief that CRC occurs only in women is erroneous. Men are commonly impacted by CRC and its many resulting effects as well.
It is not only the presence of these disease-causing fungal organisms that results in illness. Symptoms are often the result of the body's allergic response to the organisms. It is this chronic Candida infection mixed with the body's allergic response to the organisms that results in Candida Related Complex. Asthma, otitis, colitis, fungal infections such as athlete's foot, eczema, Chronic Fatigue Syndrome, cystitis, ADHD and many other conditions can be the direct result of CRC. Every child that has had repeated courses of antibiotics, often to treat ear infections, should be considered a suspect for CRC especially when the child presents with conditions that appear to be allergy-based.
Yeast can result in prostate infections in men as well as chronic bladder disorders and urinary symptoms in both men and women. Seborrhea ("dandruff") and Psoriasis are common signs. Approximately 40% of psoriasis cases can be controlled with an anti-Candida program.
Itching around the vagina, or vaginitis, is often caused by yeast. It has been demonstrated that specific anti-Candida IgE antibodies can be found in the vagina illustrating that persistent vaginitis is largely the result of allergy. In much the same way that sinus problems can be due to food allergies, although there are no foods in the nose, symptoms in the vagina can be the result of an allergic response to infection elsewhere in the body. Abnormalities in the immune system can be related to chronic yeast infection. Polycystic ovaries and endometriosis are conditions that can be greatly improved through the proper treatment of Candida.
Women with recurring vaginal yeast infections that don't seem to resolve after repeated localized treatment courses may be re-infecting themselves due to the close location of the anus to the vagina. It is not difficult for yeast colonizing the digestive tract to make its way from the rectum to the vaginal area. When the intestinal reservoir of yeast is diminished, vaginal yeast infections are often controlled as well.
Allergic reactions such as hay fever, asthma, headaches, and eczema are exacerbated by chronic yeast infections. Arthritis and Systemic Lupus Erythematosus have responded in some patients to anti-fungal treatment. IBS, Colitis, and Crohn's disease are often complicated by the presence of chronic yeast, parasites, and food allergies.
Dr. Levin uses the analogy of "weeds in the garden" to explain the balance of organisms in the digestive tract. A healthy lawn is one that has been cultivated with topsoil, tilled, fertilized, watered, weeded without poisons, and seeded. This is a lawn that is both beautiful and without weeds. One can blow dandelion seeds on the lawn and though they will sprout, they cannot penetrate the interlocking root system. They are rejected and die.
When looking at the inevitable number of organisms that we swallow on a regular basis, it is the healthy bacteria in the digestive tract that should create an environment that does not support the persistence of these pathenogenic microbes. Unfortunately, antibiotics destroy good bacteria and create a perfect environment which supports the growth of undesired yeast. When the healthy bacteria are gone and the yeast takes over, we are further predisposed to other unhealthy parasites and bacteria. All of these become weeds in the garden. Unfortunately, once yeast, parasites, and harmful bacteria have all arrived to the party, an attempt to resolve the yeast infection without also resolving the parasite and bacterial overgrowth generally fails. When yeast is present, one must aggressively look for and address other organisms in order to ensure the highest possible chance of treatment success.
Healthy bacteria in the digestive tract serve a number of important functions in the body. They produce vitamins which cannot be manufactured by the body itself. They also help to control the overgrowth of pathenogenic microbes in the gut. In fact, there are more bacteria in a healthy stool than cells in the entire human body. More than 50% of the dry weight of the stool is bacteria. These bacteria defend us against many harmful organisms such as yeast.
Unfortunately, antibiotics destroy healthy bacteria and result in a welcoming environment for "weeds in the garden". At first, these weeds are like the dandelions, though these organisms quickly seize the opportunity to colonize and shift the balance in their favor. At this stage, even when the healthy bacteria are restored, it may not be enough to eradicate the well-implanted yeast. The yeast take nutrition from the environment and make waste products, which are then dumped into our bodies and are absorbed, acting as toxins or poisons. Most people can tolerate small amounts of toxins, but when a certain threshold is reached, symptoms begin and we become toxic. Headaches, intestinal problems, aches, pains, fatigue, fuzzy thinking, and nasal stuffiness are among the many symptoms that these fungal toxins may produce.
It is the body's allergic response to these organisms and the toxins they produce that generate the majority of the symptoms experienced. Once an allergic response begins, even the elimination of the majority of the yeast may not be enough to resolve symptoms. A small remaining amount becomes enough to trigger the allergic response and thus produce ongoing symptoms.
Unfortunately, much like with Lyme disease, lab testing often misses the presence of Candida infection. Testing for Candida using stool samples often yields many "false negative" results. Dr. Levin has come to the conclusion that Candida creates "roots", or fungal filaments, which anchor it strongly to the wall of the digestive tract. He believes this is a survival mechanism as the organisms could not persist if they were purged from the body. In the book The Biology of Belief by Bruce Lipton, PhD, this theory of a consciousness for self-preservation is scientifically supported. This adherence to the gut wall significantly reduces the amount of Candida that may be observed in the stool and results in these "false negative" test results.
As is seen with Lyme disease, antibody testing for Candida often yields negative results as well. This is a characteristic sign of a suppressed immune response that simply does not have the fortitude to create antibodies.
In the past, darkfield microscopy was used to observe fungal forms in the blood. Unfortunately, the practice of using darkfield microscopy by MDs and DOs in this manner has since been outlawed by CLIA, the federal agency in charge of laboratories. The technique may still be employed by chiropractors and naturopathic physicians, but they do not have the ability to prescribe the necessary antifungal agents potentially required to address the issue. Interestingly, fungal forms observed in the blood with darkfield microscopes do not persist in the blood after subsequent antifungal treatment with a systemic antifungal agent.
More recently, additional mechanisms for evaluating the presence of Candida have become available. William Shaw, PhD, the force behind Great Plains Laboratory, discovered metabolic waste products which could be identified in the urine using a test called the "Organic Acids Test". More specifically, the presence of Arabinose and Tartaric Acid, never found in healthy humans, are powerful indicators of the presence of Candida. This can often help to confirm the presence of systemic yeast when stool cultures, or other similar tests, have returned negative but suspicion of yeast involvement remains high.
There have also been additional advances in the area of Candida testing which may be helpful when yeast organisms are found in cultures. The first is the ability to identify the specific yeast species. The second is testing to determine the best possible treatment option by performing an anti-fungal drug sensitivity test. This test will look at various options available, both herbal and prescription, and suggest which may be the most effective treatment intervention for a given patient.
In looking at treatment options, Nystatin is generally considered to be a good option for treating Candida infections in the digestive tract. The major advantage of using Nystatin is the low risk of serious systemic side effects, as the drug is not systemically absorbed. Unfortunately, this characteristic of Nystatin is also its downside. It can act as a lawnmower to remove the dandelions, though it cannot get to the root system and, as a result, may not be an effective approach in the treatment of CRC after it has passed the initial stages. Once the yeast has penetrated the intestinal wall, Nystatin may be able to help clear out the intestines, but it leaves the roots behind and the yeast will simply reemerge.
Until about twenty years ago, there were few other options for the treatment of Candida. Fortunately, today, there are several oral medications that are absorbed and work their way through the blood to attack the root system and more successfully address entrenched chronic fungal infection.
Ketaconazole (Nizoral), Fluconazole (Diflucan), Itraconazole (Sporanox) and more recently Voriconazole (VFend) are some of the more common agents that can help to address CRC at a deeper level. Clotrimazole (Lotrimin) is another "azole" drug used for the treatment of yeast, though it is generally only used for external yeast infections such as vaginal infection, athlete's foot, jock itch, and ringworm and is not used to address yeast systemically in this country. Tinidazole (Tindamax) is not FDA-approved for the treatment of yeast and may not be available in an oral form strong enough to be beneficial, though it is beneficial in cases of parasites such as giardia, amoebas, and trichomonas. Metronidazole (Flagyl) is often the drug of choice for parasites and vaginal trichomonas, though it does not have any anti-Candida properties. In fact, the PDR warns that using Flagyl may promote the overgrowth of Candida. Long-term use of Ketaconazole can inhibit adrenal function and production of testicular hormones. Unfortunately, the FDA made a decision years ago to allow a single dose of Diflucan to be used for the treatment of chronic recurrent vaginitis. This decision has created a super-strain of Candida that is not only resistant to Fluconazole but to other "azole" drugs as well.
It is important to understand that while Nystatin is not absorbed and thus has a low incidence of side effects, the more systemic anti-fungal agents such as the "azoles" do bring with them a higher risk of liver toxicity and elevation of liver enzymes. It is necessary to monitor the liver closely when using these systemic agents. Given the significance of CRC on overall health, these medications offer great potential, even with the possible side effects they may bring, as long as the patient is appropriately monitored.
Other important considerations when treating CRC are the prebiotics and probiotics. Lactobacillus and Bifidus are healthy probiotic organisms that help to inhibit the overgrowth of yeast, as well as producing vitamins and conferring numerous other health benefits. Prebiotics are less commonly understood. Their purpose is to serve as fertilizer for the good bacteria. Prebiotics consist primarily of fructooligosaccha
rides (FOS) and inulin. They are indigestible carbohydrates that support the growth of the probiotics. They are in effect a form of "Miracle Gro�" for beneficial bacteria. A number of prebiotic and probiotic products are readily available.
Beyond killing yeast with an anti-microbial, any CRC treatment program should include both a probiotic and prebiotic. Dr. Levin recommends that patients use only the highest quality products among the probiotics, and that the specific product should be changed after six-to-eight weeks to provide as many different strains of probiotics as possible. Glutamine can be helpful for restoring the integrity of the bowel wall. Butyric acid can provide an energy source for the cells of the colon.
Non-prescription products which can be helpful include oregano oil, tea tree oil used topically, and high quality colloidal silver products (Note: Colloidal silver products should be obtained from manufacturers, not made at home. Attempting to make colloidal silver at home significantly increases the risk of adverse events.). These interventions are more beneficial earlier in the condition. Once the yeast is
well-entrenched, the more powerful prescription anti-fungals may be required.
Another technique that Dr. Levin finds useful is to measure RBC (red blood cell) levels of minerals. If molybdenum is low, it should be supplemented. A waste product of Candida is called "acetylaldehyde". Aldehydes affect neurological, metabolic, endocrine, and immune function. More specifically, with Candida, it is the creation of acetylaldehyde that overload the system. Molybdenum helps to break down the aldehydes produced by the yeasts so that they can be more readily excreted by the body.
Diet is another key to resolving CRC. A diet high in simple sugars nourishes the yeast organisms. A low-carbohydrate, high protein diet should be followed. The diet should restrict fruit and contain no fruit juices. Yeast in any form should be avoided. This includes fermented foods made with yeast such as wine, beer, vinegar, breads, cakes, pastries, and most cheeses. Strawberries, blueberries, raspberries, and grapes tend to become moldy and should be avoided. Even small amounts of yeast can trigger yeast allergy symptoms to emerge. Another important aspect of diet when treating yeast-related conditions is the focus on an alkaline diet which may include the incorporation of one of a number of high-quality "Green" drinks.
Not only do the symptoms of Candida Related Complex and Lyme disease have significant overlap, but often, the treatment of Lyme disease contributes to CRC. The refusal of mainstream doctors to consider Candida combined with the use of antibiotics to treat Lyme disease results in the stage being set for the development of CRC.
Anyone that takes more than four weeks of antibiotic therapy and is on the "Standard American Diet", which Dr. Levin refers to as "SAD", is likely to have Candida overgrowth. Ideally, a combination of probiotics and the anti-fungal Nystatin would be considered a protective therapy and given to everyone on antibiotics in order to minimize the risk of a more entrenched systemic fungal infection. Once CRC takes hold, more aggressive therapy is often required.
The more one understands about Candida Related Complex, the better positioned they are to work with their doctor on evaluating whether or not CRC is a part of the overall symptom picture. In a significant number of cases of people with Lyme disease, CRC plays a key role. A failure to address this likelihood undermines the overall Lyme disease treatment protocol. Successfully addressing CRC often leads to a significant improvement in overall health and wellness.
Resources:
Dr. Levin has several lectures available on CD, including one on Candida. Others include Asthma, Hypoglycemia, Food Allergy, and Intravenous Chelation Therapy. He can be contacted through his web site:
www.warrenmlevinmd.net
[email protected]
To find a doctor in your area visit the American College for the Advancement of Medicine at www.acam.org or The American Academy of Environmental Medicine at http://www.aaem.com.
The Yeast Connection For Women: A Medical Breakthrough
by William G. Crook
The Yeast Connection Handbook
by William G. Crook
The Yeast Syndrome: How to Help Your Doctor Identify & Treat the Real Cause of Your Yeast-Related Illness
by John P. Trowbridge and Morton Walker
Coping With Candida Cookbook
by Sally Rockwell
Marjorie Crandall, PhD
www.yeastconsulting.com
Warren M. Levin, MD, PLLC blends conventional and alternative medical philosophies in his private practice in Vienna, VA. Dr. Levin has found Candida Related Complex (CRC) to be a significant factor in the presentation of many chronic conditions. Dr. Levin identifies CRC as a common iatrogenic complication in the majority of people with Lyme disease and believes that it must be adequately addressed in order to return one to an ideal state of health and wellness.
Of the family of yeasts known as Candida, Candida albicans is the most common, though there are numerous species that may result in clinical symptoms. Symptoms of Candida can affect every bodily system and are often incapacitating.
The majority of practitioners in mainstream medicine today still do not recognize the importance of the presence of Candida on overall health. They often suggest that Candida is only an issue in patients that are severely immunocompromised, such as patients with HIV, cancer, or patients that have undergone chemotherapy or radiation. This perspective is quite limited and misses the majority of patients whose health is in fact impacted by Candida.
Candida Related Complex has been called the "Yeast Syndrome", the "Yeast Connection", and Thrush, among other terms. It has also been called "imaginary", "nonsense", "fraud", and "charlatanism" by those that do not understand its implications and prevalence.
Not only does Dr. Levin believe that CRC is real, often overlooked and generally under-treated, but he has found that many people with a diagnosis of Lyme disease are experiencing symptoms that are partially, or entirely, attributable to Candida Related Complex, not to Lyme disease itself. Since the mid 20th century, five major changes in Western societies have created the perfect storm for establishment of Candida Related Complex:
1. The tremendous increase in refined and processed foods, especially sugars and chemical additives.
2. The introduction - and overuse - of antibiotics.
3. The introduction - and overuse - of cortisone and its natural and artificial derivatives.
4. The introduction and widespread use of Birth Control Pills, which are supposed to be "estrogen and progesterone" combinations, but are actually artificial, synthesized foreign molecules that are very successful in preventing pregnancy. Unfortunately, they also interfere with normal hormonal balances, and produce changes in the vaginal tissues that predispose women to Candida infection.
5. The introduction- and overuse - of drugs that suppress stomach acid production, thus depriving the users of the normal killing of foreign organisms that are ingested with food (such as Candida) and also preventing the proper digestion of protein which over time leads to malnutrition, even with healthy diets.
Dr. Levin believes that CRC is a complex problem which plays a role in multiple chronic and degenerative disease syndromes. CRC is more than just a yeast infection. In fact, most often, CRC exists without the presence of an obvious yeast infection. The belief that CRC occurs only in women is erroneous. Men are commonly impacted by CRC and its many resulting effects as well.
It is not only the presence of these disease-causing fungal organisms that results in illness. Symptoms are often the result of the body's allergic response to the organisms. It is this chronic Candida infection mixed with the body's allergic response to the organisms that results in Candida Related Complex. Asthma, otitis, colitis, fungal infections such as athlete's foot, eczema, Chronic Fatigue Syndrome, cystitis, ADHD and many other conditions can be the direct result of CRC. Every child that has had repeated courses of antibiotics, often to treat ear infections, should be considered a suspect for CRC especially when the child presents with conditions that appear to be allergy-based.
Yeast can result in prostate infections in men as well as chronic bladder disorders and urinary symptoms in both men and women. Seborrhea ("dandruff") and Psoriasis are common signs. Approximately 40% of psoriasis cases can be controlled with an anti-Candida program.
Itching around the vagina, or vaginitis, is often caused by yeast. It has been demonstrated that specific anti-Candida IgE antibodies can be found in the vagina illustrating that persistent vaginitis is largely the result of allergy. In much the same way that sinus problems can be due to food allergies, although there are no foods in the nose, symptoms in the vagina can be the result of an allergic response to infection elsewhere in the body. Abnormalities in the immune system can be related to chronic yeast infection. Polycystic ovaries and endometriosis are conditions that can be greatly improved through the proper treatment of Candida.
Women with recurring vaginal yeast infections that don't seem to resolve after repeated localized treatment courses may be re-infecting themselves due to the close location of the anus to the vagina. It is not difficult for yeast colonizing the digestive tract to make its way from the rectum to the vaginal area. When the intestinal reservoir of yeast is diminished, vaginal yeast infections are often controlled as well.
Allergic reactions such as hay fever, asthma, headaches, and eczema are exacerbated by chronic yeast infections. Arthritis and Systemic Lupus Erythematosus have responded in some patients to anti-fungal treatment. IBS, Colitis, and Crohn's disease are often complicated by the presence of chronic yeast, parasites, and food allergies.
Dr. Levin uses the analogy of "weeds in the garden" to explain the balance of organisms in the digestive tract. A healthy lawn is one that has been cultivated with topsoil, tilled, fertilized, watered, weeded without poisons, and seeded. This is a lawn that is both beautiful and without weeds. One can blow dandelion seeds on the lawn and though they will sprout, they cannot penetrate the interlocking root system. They are rejected and die.
When looking at the inevitable number of organisms that we swallow on a regular basis, it is the healthy bacteria in the digestive tract that should create an environment that does not support the persistence of these pathenogenic microbes. Unfortunately, antibiotics destroy good bacteria and create a perfect environment which supports the growth of undesired yeast. When the healthy bacteria are gone and the yeast takes over, we are further predisposed to other unhealthy parasites and bacteria. All of these become weeds in the garden. Unfortunately, once yeast, parasites, and harmful bacteria have all arrived to the party, an attempt to resolve the yeast infection without also resolving the parasite and bacterial overgrowth generally fails. When yeast is present, one must aggressively look for and address other organisms in order to ensure the highest possible chance of treatment success.
Healthy bacteria in the digestive tract serve a number of important functions in the body. They produce vitamins which cannot be manufactured by the body itself. They also help to control the overgrowth of pathenogenic microbes in the gut. In fact, there are more bacteria in a healthy stool than cells in the entire human body. More than 50% of the dry weight of the stool is bacteria. These bacteria defend us against many harmful organisms such as yeast.
Unfortunately, antibiotics destroy healthy bacteria and result in a welcoming environment for "weeds in the garden". At first, these weeds are like the dandelions, though these organisms quickly seize the opportunity to colonize and shift the balance in their favor. At this stage, even when the healthy bacteria are restored, it may not be enough to eradicate the well-implanted yeast. The yeast take nutrition from the environment and make waste products, which are then dumped into our bodies and are absorbed, acting as toxins or poisons. Most people can tolerate small amounts of toxins, but when a certain threshold is reached, symptoms begin and we become toxic. Headaches, intestinal problems, aches, pains, fatigue, fuzzy thinking, and nasal stuffiness are among the many symptoms that these fungal toxins may produce.
It is the body's allergic response to these organisms and the toxins they produce that generate the majority of the symptoms experienced. Once an allergic response begins, even the elimination of the majority of the yeast may not be enough to resolve symptoms. A small remaining amount becomes enough to trigger the allergic response and thus produce ongoing symptoms.
Unfortunately, much like with Lyme disease, lab testing often misses the presence of Candida infection. Testing for Candida using stool samples often yields many "false negative" results. Dr. Levin has come to the conclusion that Candida creates "roots", or fungal filaments, which anchor it strongly to the wall of the digestive tract. He believes this is a survival mechanism as the organisms could not persist if they were purged from the body. In the book The Biology of Belief by Bruce Lipton, PhD, this theory of a consciousness for self-preservation is scientifically supported. This adherence to the gut wall significantly reduces the amount of Candida that may be observed in the stool and results in these "false negative" test results.
As is seen with Lyme disease, antibody testing for Candida often yields negative results as well. This is a characteristic sign of a suppressed immune response that simply does not have the fortitude to create antibodies.
In the past, darkfield microscopy was used to observe fungal forms in the blood. Unfortunately, the practice of using darkfield microscopy by MDs and DOs in this manner has since been outlawed by CLIA, the federal agency in charge of laboratories. The technique may still be employed by chiropractors and naturopathic physicians, but they do not have the ability to prescribe the necessary antifungal agents potentially required to address the issue. Interestingly, fungal forms observed in the blood with darkfield microscopes do not persist in the blood after subsequent antifungal treatment with a systemic antifungal agent.
More recently, additional mechanisms for evaluating the presence of Candida have become available. William Shaw, PhD, the force behind Great Plains Laboratory, discovered metabolic waste products which could be identified in the urine using a test called the "Organic Acids Test". More specifically, the presence of Arabinose and Tartaric Acid, never found in healthy humans, are powerful indicators of the presence of Candida. This can often help to confirm the presence of systemic yeast when stool cultures, or other similar tests, have returned negative but suspicion of yeast involvement remains high.
There have also been additional advances in the area of Candida testing which may be helpful when yeast organisms are found in cultures. The first is the ability to identify the specific yeast species. The second is testing to determine the best possible treatment option by performing an anti-fungal drug sensitivity test. This test will look at various options available, both herbal and prescription, and suggest which may be the most effective treatment intervention for a given patient.
In looking at treatment options, Nystatin is generally considered to be a good option for treating Candida infections in the digestive tract. The major advantage of using Nystatin is the low risk of serious systemic side effects, as the drug is not systemically absorbed. Unfortunately, this characteristic of Nystatin is also its downside. It can act as a lawnmower to remove the dandelions, though it cannot get to the root system and, as a result, may not be an effective approach in the treatment of CRC after it has passed the initial stages. Once the yeast has penetrated the intestinal wall, Nystatin may be able to help clear out the intestines, but it leaves the roots behind and the yeast will simply reemerge.
Until about twenty years ago, there were few other options for the treatment of Candida. Fortunately, today, there are several oral medications that are absorbed and work their way through the blood to attack the root system and more successfully address entrenched chronic fungal infection.
Ketaconazole (Nizoral), Fluconazole (Diflucan), Itraconazole (Sporanox) and more recently Voriconazole (VFend) are some of the more common agents that can help to address CRC at a deeper level. Clotrimazole (Lotrimin) is another "azole" drug used for the treatment of yeast, though it is generally only used for external yeast infections such as vaginal infection, athlete's foot, jock itch, and ringworm and is not used to address yeast systemically in this country. Tinidazole (Tindamax) is not FDA-approved for the treatment of yeast and may not be available in an oral form strong enough to be beneficial, though it is beneficial in cases of parasites such as giardia, amoebas, and trichomonas. Metronidazole (Flagyl) is often the drug of choice for parasites and vaginal trichomonas, though it does not have any anti-Candida properties. In fact, the PDR warns that using Flagyl may promote the overgrowth of Candida. Long-term use of Ketaconazole can inhibit adrenal function and production of testicular hormones. Unfortunately, the FDA made a decision years ago to allow a single dose of Diflucan to be used for the treatment of chronic recurrent vaginitis. This decision has created a super-strain of Candida that is not only resistant to Fluconazole but to other "azole" drugs as well.
It is important to understand that while Nystatin is not absorbed and thus has a low incidence of side effects, the more systemic anti-fungal agents such as the "azoles" do bring with them a higher risk of liver toxicity and elevation of liver enzymes. It is necessary to monitor the liver closely when using these systemic agents. Given the significance of CRC on overall health, these medications offer great potential, even with the possible side effects they may bring, as long as the patient is appropriately monitored.
Other important considerations when treating CRC are the prebiotics and probiotics. Lactobacillus and Bifidus are healthy probiotic organisms that help to inhibit the overgrowth of yeast, as well as producing vitamins and conferring numerous other health benefits. Prebiotics are less commonly understood. Their purpose is to serve as fertilizer for the good bacteria. Prebiotics consist primarily of fructooligosaccha
rides (FOS) and inulin. They are indigestible carbohydrates that support the growth of the probiotics. They are in effect a form of "Miracle Gro�" for beneficial bacteria. A number of prebiotic and probiotic products are readily available.
Beyond killing yeast with an anti-microbial, any CRC treatment program should include both a probiotic and prebiotic. Dr. Levin recommends that patients use only the highest quality products among the probiotics, and that the specific product should be changed after six-to-eight weeks to provide as many different strains of probiotics as possible. Glutamine can be helpful for restoring the integrity of the bowel wall. Butyric acid can provide an energy source for the cells of the colon.
Non-prescription products which can be helpful include oregano oil, tea tree oil used topically, and high quality colloidal silver products (Note: Colloidal silver products should be obtained from manufacturers, not made at home. Attempting to make colloidal silver at home significantly increases the risk of adverse events.). These interventions are more beneficial earlier in the condition. Once the yeast is
well-entrenched, the more powerful prescription anti-fungals may be required.
Another technique that Dr. Levin finds useful is to measure RBC (red blood cell) levels of minerals. If molybdenum is low, it should be supplemented. A waste product of Candida is called "acetylaldehyde". Aldehydes affect neurological, metabolic, endocrine, and immune function. More specifically, with Candida, it is the creation of acetylaldehyde that overload the system. Molybdenum helps to break down the aldehydes produced by the yeasts so that they can be more readily excreted by the body.
Diet is another key to resolving CRC. A diet high in simple sugars nourishes the yeast organisms. A low-carbohydrate, high protein diet should be followed. The diet should restrict fruit and contain no fruit juices. Yeast in any form should be avoided. This includes fermented foods made with yeast such as wine, beer, vinegar, breads, cakes, pastries, and most cheeses. Strawberries, blueberries, raspberries, and grapes tend to become moldy and should be avoided. Even small amounts of yeast can trigger yeast allergy symptoms to emerge. Another important aspect of diet when treating yeast-related conditions is the focus on an alkaline diet which may include the incorporation of one of a number of high-quality "Green" drinks.
Not only do the symptoms of Candida Related Complex and Lyme disease have significant overlap, but often, the treatment of Lyme disease contributes to CRC. The refusal of mainstream doctors to consider Candida combined with the use of antibiotics to treat Lyme disease results in the stage being set for the development of CRC.
Anyone that takes more than four weeks of antibiotic therapy and is on the "Standard American Diet", which Dr. Levin refers to as "SAD", is likely to have Candida overgrowth. Ideally, a combination of probiotics and the anti-fungal Nystatin would be considered a protective therapy and given to everyone on antibiotics in order to minimize the risk of a more entrenched systemic fungal infection. Once CRC takes hold, more aggressive therapy is often required.
The more one understands about Candida Related Complex, the better positioned they are to work with their doctor on evaluating whether or not CRC is a part of the overall symptom picture. In a significant number of cases of people with Lyme disease, CRC plays a key role. A failure to address this likelihood undermines the overall Lyme disease treatment protocol. Successfully addressing CRC often leads to a significant improvement in overall health and wellness.
Resources:
Dr. Levin has several lectures available on CD, including one on Candida. Others include Asthma, Hypoglycemia, Food Allergy, and Intravenous Chelation Therapy. He can be contacted through his web site:
www.warrenmlevinmd.net
[email protected]
To find a doctor in your area visit the American College for the Advancement of Medicine at www.acam.org or The American Academy of Environmental Medicine at http://www.aaem.com.
The Yeast Connection For Women: A Medical Breakthrough
by William G. Crook
The Yeast Connection Handbook
by William G. Crook
The Yeast Syndrome: How to Help Your Doctor Identify & Treat the Real Cause of Your Yeast-Related Illness
by John P. Trowbridge and Morton Walker
Coping With Candida Cookbook
by Sally Rockwell
Marjorie Crandall, PhD
www.yeastconsulting.com
About the author
Scott Forsgren (Author) is a health writer, advocate, and coach. He is the editor and founder of BetterHealthGuy.com where he shares his now 17 year journey through the world of Lyme disease and the myriad of factors that it often entails. He has been fortunate to have written for publications such as the Public Health Alert, Explore!, Bolen Report, and Townsend Letter. Scott expresses gratitude for the information shared by Dr. Neil Nathan and Dr. Wayne Anderson in support of this article. More information on his work is available at http://www.BetterHealthGuy.com.
latest posts

tags
Cowden Protocol month 1

23andMe genetic Testing
Disclaimer: The information on this website is not a substitute for professional medical advice.
Always consult with your treating physician before altering any treatment protocol.
Always consult with your treating physician before altering any treatment protocol.
