Morgellons: Update On The Mysterious Disease
July 24, 2014 in Science/Research by Ginger Savely, RN, FNP-C

Itching, biting, stinging and crawling sensations with open sores and unusual objects oozing out of your skin. Sounds like a nightmare, doesn’t it? Or an episode of X-Files?
This is not the fantasy plot of a television show that focuses on the bizarre and other-worldly. It is the living nightmare of thousands of people across the United States suffering from an illness known as Morgellons disease. California, Texas and Florida are, in descending order, the states where clusters of the disease are reported most frequently. Most other states and several other countries also have victims who have registered their cases on www.morgellons.org, the web site of the not-for-profit Morgellons Research Foundation. Of interest to nurses is that their profession represents one of the highest percentage of reported sufferers.
An “orphan” disease, without a known cause, diagnostic test or cure, Morgellons disease is not recognized by the state health departments or the Centers for Disease Control and Prevention (CDC), although reports of patients with the symptoms go back over 300 years. The diagnosis, at this point, is based upon a patient fitting the symptom criteria.
There are a few dozen symptoms that all or most sufferers share in common. These include, but are not limited to, profound fatigue, anxiety, insomnia, joint and muscle pain, hair loss, cognitive disturbances (such as loss of short term memory, inability to concentrate or comprehend), disfiguring lesions, blue, white, red and black fibers poking up through the skin, black specks and “fuzz balls” on the clothes and skin, objects racing across the eyes, and hyperpigmented scars when the lesions heal. Worst of all is the constant and unnerving aggravation of feeling as though there are bugs or worms crawling through one’s body, biting, stinging and causing insupportable itching and discomfort.
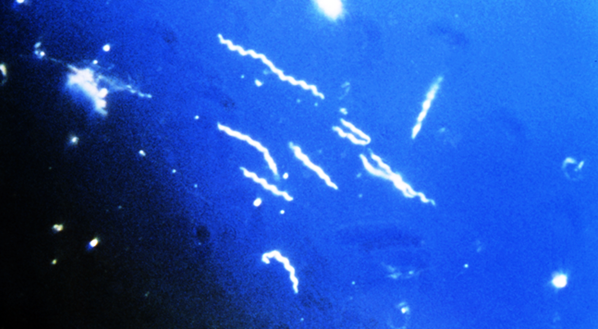
As a nurse practitioner interested in unusual infectious diseases, I have now seen over one hundred Morgellons patients in my San Francisco practice. I am intrigued by the consistency of the patients’ stories and the mysterious nature of the disease. Most victims seem to have already been immunosuppressed in some way before noticing the onset of their symptoms. People on immunosuppressive therapy, AIDS patients and those with chronic (often undiagnosed) tick-borne diseases seem to be particularly susceptible. A majority of the afflicted report exposure to stagnant or polluted water or to dirt entering the skin, such as by a splinter or while gardening without gloves, prior to the initiation of their symptoms.
The causative organism of Morgellons disease remains a medical mystery. Randy Wymore, PhD of the Oklahoma State University Center for Health Sciences in Tulsa, Oklahoma, is the Director of Research of the Morgellons Research Foundation. Dr. Wymore is examining the fibers, scabs and other samples from Morgellons patients and to date his preliminary research suggests that the fibers are not merely textile contaminants and that the scabs have qualitative differences from the scabs of unaffected individuals. Research is underway with the goal of discovering the etiology of the disease and identifying concrete diagnostic criteria.
Meanwhile, pending more understanding of the etiology and risk factors, a cure is elusive. Treatment focuses on symptom management and, when a patient is willing (and most are), treatment with experimental combinations of antibiotics, antifungals and antiparasitics. Many have improved with treatment but not without enduring temporary symptom intensification and the need for frequent medication changes due to an apparently uncanny ability of the organism to adapt or mutate. Every patient is unique, and so treatment involves trial and error and months of frustration for both the patient the practitioner.
Not all Morgellons patients are lucky enough to improve with the experimental treatments. One such patient was a 23 year old male patient of mine who recently chose to end his life of suffering and despair. His untimely death serves to highlight the seriousness of the disease and the urgency for a proper diagnosis and cure.
The first step to understanding this medical mystery is acceptance of the disease as a real entity. We must avoid the temptation to hastily categorize these patients as delusional, which is happening in medical offices around the country every day. When patients present with unusual symptoms, it is unjust to summarily discount them and relegate them to the psychiatrists’ office without a thorough and proper history and exam.
If health care providers would take the time and effort to really look at these patients’ skin with illuminated magnification, they would be amazed and confounded by the unusual things they would see.
The history of medicine is replete with instances of infectious diseases that are misdiagnosed as psychosocial problems. Gastric ulcer patients were told that their inability to handle stress was the cause of their disease, epileptics were believed to be possessed by the devil, and patients with tertiary syphilis were placed in straight jackets in insane asylums.
When patients present with unusual and unbelievable symptoms, health care providers would do well to make sure that they are treated with the dignity, attention and respect that they deserve.
Suggested reading:
For further information about Morgellons disease please visit www.morgellons.org, the website of the Morgellons Research Foundation
This is not the fantasy plot of a television show that focuses on the bizarre and other-worldly. It is the living nightmare of thousands of people across the United States suffering from an illness known as Morgellons disease. California, Texas and Florida are, in descending order, the states where clusters of the disease are reported most frequently. Most other states and several other countries also have victims who have registered their cases on www.morgellons.org, the web site of the not-for-profit Morgellons Research Foundation. Of interest to nurses is that their profession represents one of the highest percentage of reported sufferers.
An “orphan” disease, without a known cause, diagnostic test or cure, Morgellons disease is not recognized by the state health departments or the Centers for Disease Control and Prevention (CDC), although reports of patients with the symptoms go back over 300 years. The diagnosis, at this point, is based upon a patient fitting the symptom criteria.
There are a few dozen symptoms that all or most sufferers share in common. These include, but are not limited to, profound fatigue, anxiety, insomnia, joint and muscle pain, hair loss, cognitive disturbances (such as loss of short term memory, inability to concentrate or comprehend), disfiguring lesions, blue, white, red and black fibers poking up through the skin, black specks and “fuzz balls” on the clothes and skin, objects racing across the eyes, and hyperpigmented scars when the lesions heal. Worst of all is the constant and unnerving aggravation of feeling as though there are bugs or worms crawling through one’s body, biting, stinging and causing insupportable itching and discomfort.
As a nurse practitioner interested in unusual infectious diseases, I have now seen over one hundred Morgellons patients in my San Francisco practice. I am intrigued by the consistency of the patients’ stories and the mysterious nature of the disease. Most victims seem to have already been immunosuppressed in some way before noticing the onset of their symptoms. People on immunosuppressive therapy, AIDS patients and those with chronic (often undiagnosed) tick-borne diseases seem to be particularly susceptible. A majority of the afflicted report exposure to stagnant or polluted water or to dirt entering the skin, such as by a splinter or while gardening without gloves, prior to the initiation of their symptoms.
The causative organism of Morgellons disease remains a medical mystery. Randy Wymore, PhD of the Oklahoma State University Center for Health Sciences in Tulsa, Oklahoma, is the Director of Research of the Morgellons Research Foundation. Dr. Wymore is examining the fibers, scabs and other samples from Morgellons patients and to date his preliminary research suggests that the fibers are not merely textile contaminants and that the scabs have qualitative differences from the scabs of unaffected individuals. Research is underway with the goal of discovering the etiology of the disease and identifying concrete diagnostic criteria.
Meanwhile, pending more understanding of the etiology and risk factors, a cure is elusive. Treatment focuses on symptom management and, when a patient is willing (and most are), treatment with experimental combinations of antibiotics, antifungals and antiparasitics. Many have improved with treatment but not without enduring temporary symptom intensification and the need for frequent medication changes due to an apparently uncanny ability of the organism to adapt or mutate. Every patient is unique, and so treatment involves trial and error and months of frustration for both the patient the practitioner.
Not all Morgellons patients are lucky enough to improve with the experimental treatments. One such patient was a 23 year old male patient of mine who recently chose to end his life of suffering and despair. His untimely death serves to highlight the seriousness of the disease and the urgency for a proper diagnosis and cure.
The first step to understanding this medical mystery is acceptance of the disease as a real entity. We must avoid the temptation to hastily categorize these patients as delusional, which is happening in medical offices around the country every day. When patients present with unusual symptoms, it is unjust to summarily discount them and relegate them to the psychiatrists’ office without a thorough and proper history and exam.
If health care providers would take the time and effort to really look at these patients’ skin with illuminated magnification, they would be amazed and confounded by the unusual things they would see.
The history of medicine is replete with instances of infectious diseases that are misdiagnosed as psychosocial problems. Gastric ulcer patients were told that their inability to handle stress was the cause of their disease, epileptics were believed to be possessed by the devil, and patients with tertiary syphilis were placed in straight jackets in insane asylums.
When patients present with unusual and unbelievable symptoms, health care providers would do well to make sure that they are treated with the dignity, attention and respect that they deserve.
Suggested reading:
- Savely, GR. Leitao. M. Skin Lesions and Crawling Sensations: Disease or Delusion? ADVANCE for Nurse Practitioners, May 2005, 16-17.
- Savely, GR, Leitao, M, Stricker, RB. The Mystery of Morgellons Disease: Infection or Delusion? American Journal of Clinical Dermatology 2006; 7(1):1-5.
For further information about Morgellons disease please visit www.morgellons.org, the website of the Morgellons Research Foundation
About the author
latest posts

tags
Cowden Protocol month 1

23andMe genetic Testing
Disclaimer: The information on this website is not a substitute for professional medical advice.
Always consult with your treating physician before altering any treatment protocol.
Always consult with your treating physician before altering any treatment protocol.
