Interview: Dr. Murray Susser, MD, Partnering With Patients: A Team Approach (part 1)
March 1, 2009 in Interviews by Tina J. Garcia, with Dr. Murray Susser, MD

It has been said that there is a silver lining in every dark cloud. I always believed that to be true; however, it wasn’t until I was overcome by the dark clouds of Lyme disease infection, that I was able to actually experience this phenomenon. For, if I had not contracted a debilitating Lyme infection from a tick bite, I would not have been fortunate enough to meet Dr. Murray Susser and his warm and radiant wife, Phyllis.
I feel greatly blessed through acquiring such cherished friendships in my association with the Lyme community. Dr. Susser has exhibited thoughtful medical care, compassion, generosity and friendship, and it was most memorable for me to peer through his panoramic window of medical experience during this interview. May I present the delightfully comical and impressive, Dr. Murray Susser.
Tina: So, Dr. Susser, it is also said that the journey of a thousand miles begins with the first step. With regard to your journey through medicine, would you please tell us what that first step was for you?
Dr. Susser: Yes. I graduated from the University of Pittsburgh Medical School in 1966. I went into family practice and very quickly, within the first year, I realized that medicine didn’t work the way I wanted it to. In other words, it wasn’t to my satisfaction. I started looking for alternative solutions, because people weren’t getting better. I tried a lot of different things, and finally, I stumbled onto Vitamin E. A friend of mine kept bugging me to read a book called Vitamin E for Ailing and Healthy Hearts by Wilfrid E. Shute, M.D. At the time I told my friend, “This is a quack book, but I’ll read it if you promise to never ask me about vitamins again.”
So, I read the book and Shute talked about treating 30,000 people with Vitamin E and all the great results he had with scar tissue, heart disease, high blood pressure, venous disease and blood clots, impotency and sexual dysfunction and all sorts of various disorders. At first I thought this guy must have been confabulating or was Baron von Munchausen.
Around that time, a patient came to see me who had suffered with venous disease of her legs for thirty years and had seen many doctors. She had terrible varicose veins that would develop infection and swelling andphlegmasia alba dolans. Phlegmasia means swelling, alba means whitish and dolans means pain. So, she had white, swollen, painful legs. If you just touched them with your finger, she would scream. There is a test, the Richardson test, where you wrap a blood pressure cuff around the leg and inflate the cuff, and note when it becomes painful. Well, when I put the cuff around her leg, she screamed, so I couldn’t even puff it up.
So, I asked her about all the ordinary things that could be used and she had used all of them and none of them had worked. Then I remembered Wilfrid Shute had said Vitamin E 800 units a day. So, I sent her to the drug store to get 800 units a day of Vitamin E, and she started doing that. When she came back in three weeks, she was almost cured! I was stunned! When I put the blood pressure cuff around her leg, I ran it up to the top, 300 milliliters of mercury and there was no pain. I was really excited and thought, “This cannot be a coincidence; this is a miracle.” The funny thing is, the woman wasn’t the least bit surprised and almost not appreciative. She just thought I was doing my job by getting her better.
I followed her for a couple months more and she was virtually cured with 800 units of Vitamin E a day. At the time, 800 units scared me, because I thought it was a high dose. I now sometimes put people on 20,000 units and I’ve had good results doing that. And I have a patient now who has been getting an epidural injection for spinal pain every two months for years. I started her on 10,000 units of Vitamin E a day and she’s worked up to 17,000 units, but she’s now gone eleven months without an epidural.
Now Vitamin E doesn’t work too well on nerve pain, but does work on bruises, soft tissue pain, sunburn and spider and insect bites very well. It also works for post-accident, soft-tissue injuries. So, they called me the “Vitamin E King” because I’ve used so much Vitamin E.
And all this business about Vitamin E being dangerous was the biggest propaganda of all time. It was based on a meta analysis, which is a study in which you take a bunch of lousy studies, put them together in a statistical manner and statistically maneuver it, to show that you compare some parameter with the treatment you’re interested in. So, I think the way they did it was with twenty-some studies comparing patient death with the amount of Vitamin E they took. That wasn’t only what the study was about; that was the data in the study. They took the seven studies with the highest death rates and found out how much Vitamin E these people were using and they found that these people were using more Vitamin E than the other studies. So, they said that high Vitamin E was related to high death rate. Then they published that study as if it were factual, but it was skewed. You know what Mark Twain said about statistics--that there are three kinds of lies—there are lies, damn lies and there are statistics.
It’s just like the Bible; the Devil can quote scripture to suit his purpose. So, anyhow, I got into Vitamin E and that opened the door for me. Then I started to look for more and more alternatives. And I was very excited. On my regular hospital rounds, I went into the doctors’ dining room where I went every day for lunch. I said, “Hey! Look what I found!” And all the doctors told me it was nonsense. They said, “Oh, Susser, you’re crazy! It was just coincidence!” But it wasn’t coincidence; it was way, way out of the realm of coincidence. They couldn’t believe that Vitamin E could be that powerful.
I saw it happen, so I knew it was true. That started me on my odyssey in nutrition. I saw a lot of surprising things happen. I had one guy who was scheduled to have a heart transplant, in the early days of heart transplants, when patients would live for a week afterwards at most. He got mad and walked out of the hospital, because he was waiting for a donor. He came to see me and said, “I don’t have long to live. Put me on something, some Valium maybe.” I asked him if he wanted to try some Vitamin E. He said, “What’ve I got to lose?”
So I put him on Vitamin E, and a year later he was playing golf and carrying his clubs without a cart! He never had a heart transplant, never had heart surgery, and he was fine for a long, long time. Then shortly after that, he called with an emergency saying he had stomach pain. It was the day after Thanksgiving and he said he ate too much turkey. I thought it may have been his heart, so I put him in coronary care. He insisted that it was his stomach, but I didn’t want to take any chances with him.
So I had Brian Kennedy, my cardiology friend, see him. Kennedy said, “This is an amazing case. This guy was supposed to have a heart transplant. He should have been dead a long time ago.” I said, “Well, Brian, what do you think of vitamin E?” And he walked away. And he was a good friend. But he couldn’t see the possibility that Vitamin E could have done this.
Tina: It’s really hard for some doctors to “cross over” isn’t it?
Dr. Susser: Well, it wasn’t too hard for me. A lot of doctors see it and they don’t believe it. They’re afraid to think outside the box. Remember, I was a jet fighter pilot -- now we’re talking fear.
Tina: Is it something one picks up in medical school that causes this denial?
Dr. Susser: But seriously, I think it has to do with the way we’re brought up. I had a lonely upbringing. My father was estranged and had a bad accident when I was younger and my mother was busy working and taking care of the family. She was too busy to pay much attention to me. I was the youngest of five. Nobody paid much attention to me, and I had to grow up on my own. I didn’t have a lot of dogma telling me how to live in the world. So, I had to learn everything myself. I had a good brain, I always made good grades, I had a good memory and I could learn quickly.
I grew up in a very smart family, everyone was very smart. So, I did things in my own way. It’s not a big leap of faith for me to see something that’s not in the conventional box. So, what I wound up doing, which was really most interesting and satisfying to me, was to treat people who slipped through the cracks of conventional medicine.
First I learned about Vitamin E and then I read Linus Pauling on Vitamin C. I saw the miracles with Vitamin C, too. I read Adele Davis who was a great nutritional guru who wrote some great books around that time. I got her on the phone and she was excited to hear from an M.D. who was interested in nutritional medicine. I went to a convention in San Francisco , where I met her, and she became my mentor. I started using vitamins according to what she wrote in her books and I learned about other nutritionists around the country, such as Carlton Fredericks, whom I could call.
These great nutritionists were all marginalized by conventional medicine. They were all considered quacks and attacked in various ways by the media. I kept a low profile and just did my nutritional stuff, and then I went to a meeting and learned abut hypoglycemia from Harold Harper and Carlton Fredericks. Conventional docs thought that hypoglycemia was another non-disease, a notion. Hypoglycemia is very real.
Tina: Was there testing for it at the time?
It was hard to test; it was a clinical diagnosis. You can do a glucose tolerance test and find hypoglycemia, but it’s a miserable test. The conventional docs wouldn’t agree to it, though. Hypoglycemia was defined as having blood sugar below 40, but your average blood sugar was 65 to 115. Now they’ve made it 65 to 99, which means that the American Diabetic Association can get more people called diabetic. They keep lowering the levels. For instance, blood pressure of 140 was considered borderline. Now, 120 over 80 is considered normal and 121 is now considered pre-hypertensive, so they can give hypertensive drugs much sooner.
Anyhow, I started learning about hypoglycemia. The normal hypoglycemic level of 65 is way too low; the normal should not be less than 90 or 85. They call 65 the low normal and they call 40 hypoglycemia. So, what is it if it’s between 40 and 65? I was at an affair at the medical school and I saw Dr. Fielding, who was our Chief Endocrinologist and my endocrinology professor while I was in medical school. So, I said, “Dr. Fielding, I have a question about blood sugars. If 65 is the low normal and 40 is hypoglycemia, what is 50?” And he answered, “Borderline.” You mean that whole realm from 40 to 65 is borderline and 70 is normal?
So, it was considered a non-disease and never treated. In fact, the New England Journal of Medicine published an editorial on the epidemic of a non-disease called hypoglycemia. It’s really a form of malnutrition and has to do with all sorts of problems including depression, anxiety, confusion--and obesity is very much related to hypoglycemia. So I went from disease to disease just like that. Then I learned about chelation and treated vascular disease with intravenous chelation and became experienced and successful doing that. This helped a lot of people and I had a lot of success with patients using chelation.
Tina: I had a primary care physician once who refused to consult with my Lyme doc, because my Lyme doc used chelation. The PCP surprised me by telling me that he signed a promise or statement when he finished medical school that he would never use chelation. I thought that was outrageous.
Dr. Susser: Chelation wasn’t that popular when I graduated, but that’s almost violating something in the Constitution. I think that’s an unconstitutional thing to do. I can’t imagine a medical school would do that.
Chelation means metal-binding. It was originally used, and is still used, for heavy metal poisoning. However, in conventional medical wisdom, chelation is only used for heavy duty metal poisonings. That would mean a lethal amount from a laboratory or an industrial accident, or if a child gets into a bucket of paint or eats paint chips, or someone swallows mercury. The chelators used would be EDTA or BAL, which is a mercury chelating agent.
These chelators bind lead, cadmium, mercury, tin, silver and nickel. The most toxic metals we deal with are mercury, lead and cadmium. It’s interesting that mercury wasn’t even discovered as a toxin until about twenty years ago. When I used to do hair analysis and I’d find high mercury, I would wonder what that would mean. No one seemed to know. Then Hal Huggins did some important work with mercury in his dentistry practice in Colorado , and he came up with some of the first discoveries of low-level mercury as a poison.
The poisonous level we’re talking about is several orders of magnitude below the laboratory and industrial poisoning. It’s a low-grade, insidious poisoning that poisons our arteries, our brains and our endocrine and immune systems.
Tina: Which is really important in our day and age, right? Aren’t we being bombarded with these toxic metals?
Dr. Susser: Well, improvements have been made, such as removing lead from paint, gasoline, solder and pipes. We used to have a lot of exposure to lead, but we’ve decreased it enormously. It is still too much, though. Mercury has been a major problem, but they’re decreasing that. Except now all the new light bulbs will have mercury in them and that’s going to cause a mess. There is still lead in some of our water pipes, and there are other industrial sources as well. Breathing gasoline fumes and getting gasoline on your skin can cause exposure to lead, also.
A big source of mercury is fish like tuna and swordfish, which are heavily loaded with it. Silver amalgam fillings in teeth are fifty percent mercury and we’re getting a lot of mercury from those. Many dentists are stopping this practice, but the American Dental Association has managed to keep them legal and is still saying that silver-mercury amalgams are a valid thing to do. There are some countries now which are banning these amalgams, especially in pregnant women and children. I think Sweden , Finland , Germanyand other parts of the world are starting to ban mercury fillings in certain populations, but there is a lot of legality involved in all of that.
Mercury also comes from the fumes of power plants that burn coal and other fossil fuels. So, if you’re near a power plant that’s spewing out smoke, it’s probably pretty polluted. There are silver-mercury batteries and mercury switches in our walls and lights. We’ve gotten rid of mercury thermometers, so that helps. The heavy metal picture is probably, overall, getting better. However, chelation is something that can be a real deterrent to accumulating these metals.
Tina: I’ve heard that chelation works on plaque in arteries.
Dr. Susser: As a doctor who uses chelation, I legally can’t say that chelation works on arteries. I can tell you that my experience is that chelation takes cadmium and lead out of the arterial wall, and cadmium and lead, and mercury to some extent, are known to block the action of nitric oxide. Nitric oxide opens arteries and is blocked by these heavy metals. Therefore, logically, you would think that by blocking the nitric oxide, your arteries would tend to clamp down, spasm, close up and cause damage. Nitric oxide is a natural substance in our bodies that is made in large part from arginine, which is an amino acid. So, taking amino acids is a good way to open up your arteries. We’ve found that arginine is very helpful in high blood pressure, because high blood pressure will result from lack of nitric oxide.
Chelation is really wonderful in many ways. It cleans out these toxic elements in your body. It may be hard not to eat tuna fish, swordfish, halibut, king mackerel and even orange roughy is pretty high in mercury. This is interesting; you know, the safest fish you can eat is wild salmon, because it has beautiful oils and it has almost no mercury because it eats krill. Krill does not accumulate mercury. Whereas, farm salmon eat small fish and small fish have mercury in them. The more fish they eat, the more mercury they accumulate. This is called biomagnification. So, farm salmon biomagnify the mercury like any other big fish.
If you don’t study it, it’s hard to know what’s safe to eat. I still love tuna sushi and I know when I’m eating the mercury it’s not good for me, but I take a lot of oral chelators, such as EDTA and DMSA. Now, oral is not as good as intravenous chelation, because all the oral chelators have to go through the liver where they use up most of their chelation by taking toxic metals out of the liver. That’s very good for you, but it doesn’t help the muscles or your other organs very much. If you take the oral chelation long enough, maybe years or decades, and get your liver completely cleaned out, then you start getting the other parts of your body. These heavy metals have a long half-life in the body. Lead, cadmium and mercury probably have a half-life of between twenty and twenty-five years. That means that, if you have twice as much lead in your body as you’re supposed to have and if you don’t do anything to get rid of it, it will take your body twenty years or more to get it down to the ideal level. That is, so long as you don’t add any more.
Tina: How do you integrate all this knowledge in your approach to patients?
Dr. Susser: My current practice is using all the elements that I’ve used over the years and I’ve found that the disease that is the most damaging, the most prevalent that slips through the cracks of conventional medicine the most, is Lyme disease. Lyme disease is rampant in the east and it is becoming more and more prevalent in the west. It was discovered in Lyme , Connecticut ; that’s where the name came from, where they first described the disease in this country. It’s a tick-borne disease--that’s what it’s famous for.
These are Ixodes ticks which bite this certain kind of deer that are common on the east coast. These deer are often infected with Lyme and other bacteria that can be carried by ticks. So, there’s Lyme and the co-infections. The co-infections are Babesiosis, Erlichiosis, Bartonella, Brucellosis, mycobacteria, and of course, ticks carry the rickettsial diseases like Rocky Mountain Spotted Fever. So, there are a lot of things you can get from a tick bite, and some ticks will carry two and three different bugs when they bite you. They used to say that one tick out of a hundred would carry Lyme, but now they’re saying one tick out of two will carry the disease.
If you get a tick bite, there’s a high likelihood of getting Lyme disease. If you do get a tick bite, get the head of the tick out with a little pair of pliers. Some people say you can cook it out of there, but that doesn’t work. A good thing to do is to save the tick, freeze it or put it in formaldehyde and have it tested. In the meantime, I would take antibiotics for three to four weeks and maybe longer, just in case, because the likelihood of infection is too high.
Tina: This protocol is entirely different than the Infectious Diseases Society of America treatment guidelines, which recommend only 200 mg of Doxycycline with the fulfillment of some absolutely ludicrous attachment and endemic criteria. I would take your treatment over theirs any day.
Dr. Susser: Yes, they’re really out of touch, really out of touch. The Infectious Diseases Society of America has been accused of having conflicts of interest. The IDSA panel made the announcement that chronic Lyme disease doesn’t really exist, and it turns out they probably had financial interests with insurance companies. The Attorney General of Connecticut brought charges against them.
My approach to patients is one of partnership in helping with their diseases. I am the junior partner; the patient is in charge. I will be the best advisor I can possibly be. I will offer options, because most of the things that I do don’t have rigid protocols. Like the old days--strep throat, ten days of penicillin or pyelonephritis, seven days of Keflex. There are a lot of rigid protocols in medicine and most of the things I work with are conditions like chronic fatigue syndrome, which is one that falls through the cracks. It was mostly considered to be an emotional disorder or depression. I’d say that if you had your life taken away by an illness, wouldn’t you be depressed?
So, this book I wrote twenty years ago on Chronic Fatigue Syndrome is still valid in many ways, because the principles contained within it are what I apply to my patient approach. I look at all the possibilities and offer what certainty I can to patients. One of my strengths in medicine is that I’m willing to live with uncertainty and most doctors are not.
For example, one thing that I know is that something caused your disease, but I don’t know what it is. It has to be in some category or another—a bacteria or a toxin or allergy. So, I take the most likely possibility and design a good safe therapeutic trial and do that. Now, with Lyme, the testing has recently given us much more certainty, with Igenex Lab and tests like the CD57. There are a number of things that give us much more information about Lyme.
So, I had a patient just today who had her tick bite twenty-some years ago, with a bull’s eye rash and everything, and she’s probably been to fifteen doctors, none of whom would believe she has Lyme. She has Lyme tests from labs that don’t do well with Lyme and they came back equivocal or negative, so she didn’t have Lyme by any standard for all these years. Yet, she has all the classic signs of Lyme—myalgia, arthralgia, brain fog, classical rash in New York , and her mother recognized it. She has Lyme clinically. In two weeks, if the testing comes back positive, there’s a ninety-six percent chance she has Lyme. I say that, just from her clinical history, there is a ninety-nine percent chance she has Lyme, no matter what the test shows. She’s been sick all these years.
I even use the principals of Thomas McPherson Brown, who was the great rheumatologist at George Washington University Medical School . He discovered that he could cure sixty percent of his rheumatoid arthritis patients by giving them minocycline, an antibiotic, for ten months. He found Chlamydia in the joints of rheumatoid arthritis patients, which is a bacterium. He didn’t know anything about nutrition or probiotics and he was a major player in conventional medicine. He published in peer reviewed journals, and not only that, he was in Washington , D.C. and was the rheumatologist for three different presidents in White House. This guy was big time and he was ignored by conventional medicine. It’s one thing if they ignore me here in my little office, but to ignore Thomas McPherson Brown is really insane. I now have seen many patients who came to me with a diagnosis of rheumatoid arthritis; I discovered Lyme and treated them successfully – no more rheumatoid arthritis!
Tina: Have you ever treated a patient who presented with a bull’s eye rash?
Dr. Susser: Yes, and I treated the patient for three weeks, and they never got Lyme. And, of course, the earlier the diagnosis, the easier it is to treat.
Tina: Are you finding Lyme cases here in Arizona ?
Dr. Susser: I treat patients who acquired Lyme in other states, and I have patients who travel from northernCalifornia , Utah , New Mexico and Florida . As for Arizona , absolutely, quite a few. Most of them have been around for a long time, months or even years. I’ve seen acute cases, but curiously enough, not with a tick bite. There are other insects that might carry it, maybe fleas, mites, mosquitoes or houseflies. There are definitely more mammals than deer who carry it, like mice and squirrels and rabbits. And I know horses and dogs can get it, too. So, there are many animals that carry Lyme and it’s getting more and more prevalent. At the same time, we don’t have any really good answers for it. The antibiotics are a poor answer for it, but at least if you catch it early, it can work very well.
CFS is another disease that slips through the cracks. It was first named by Paul Cheney and Dan Peterson in Incline Village , Nevada . They had a flu epidemic and some of the people remained sick. That was the time when the Epstein Barr test first became available on the clinical market. All these people began testing positive for Epstein Barr and they decided it was an Epstein Barr epidemic, which it turned out not to be. It turns out that Epstein Barr, which is Human Herpes Virus 4, is in all of us and when you get a serious illness, the HHV4 virus flares.
That led to confusion between Epstein Barr and CFS. When they found out that CFS was not caused by EBV, they decided it was an emotional disease and a form of depression. It was a crippling disease and in some cases it probably was Lyme. The definition of CFS is fifty percent debility for greater than six months with no known cause. It also has other symptoms like muscle pain, joint pain and swollen glands. So, myalgia was a common accompaniment.
In my book that I wrote with Michael Rosenbaum, called Solving the Puzzle of Chronic Fatigue Syndrome, I came up with the idea prior to that of Mixed Infection Syndrome. Again, the wisdom of conventional medicine is that you can only have one infection at a time until you’re dying, and then you can have all these opportunistic infections that take hold. In my opinion, “opportunistic” is a redundant word, because all infections are opportunistic. They look for the opportunity to invade. What they mean is that an infection needs a real strong opportunity.
We are constant besieged with bacteria and various organisms in the body. There are five hundred different bacteria that live in the gut. There are hundreds that live in the mouth, live under our fingernails and live on the skin. So, we have many different bacteria. The total count in the gut is variable. Some people say it’s three trillion and some people say it’s much more than that. How do you count them; it’s hard.
The point is that in CFS as a diagnosis, it will disappear when we are smart enough to diagnose all the different infections and all the different toxicities that can cause chronic fatigue. Lyme is a perfect example. Lots of these people we’ve labeled with CFS have Lyme disease. When we discover the Lyme disease, it’s no longer CFS; it’s chronic fatigue from Lyme disease. If they also have Babesia or some other co-infection, it’s Mixed Infection Syndrome. They commonly have been on antibiotics for one reason or another and get an overgrowth of yeast in the gut. Then they have some sort of fungal or yeast infection. Then that opens the door to parasites and to other forms of bacteria that can invade, such as clostridium dificile and things of that nature. So, there are a number of organisms that will invade under these circumstances, and the patient is not terminal. The immune system is not totally collapsed. It’s just collapsed enough. Then there are confounding factors like toxic metals and toxic fungus and molds in the house. One good thing about Lyme and the co-infections is that they validate my theory from twenty years ago that we get mixed infections.
A leaky roof or a leaky water pipe will lead to black mold, one of which is Stachybotrys. Stachybotrys toxins can be crippling and can lead to chronic fatigue and immune system depletion. Then the yeast, bacteria and parasites can invade. So, I would consider all these things in a patient with CFS symptoms, but not necessarily test for all of them. When you start testing for all these things, you run out of blood and money pretty quick. If I tested for all the things that are possible, I could drain somebody’s bank accountand their whole vascular system. Therefore, I use my best clinical judgment, and I have a lot of experience doing that.
Tina: What would you say is the difference between Chronic Fatigue and Fibromyalgia?
Dr. Susser: Aside from the fact that they commonly occur together, it is a case of which came first—the chicken or the egg—fibromyalgia means muscle pain and chronic fatigue is just that, chronic fatigue. You can have one without the other, but they commonly occur together. Fibromyalgia is fatiguing, and some people start off with fatigue and the fibromyalgia follows.
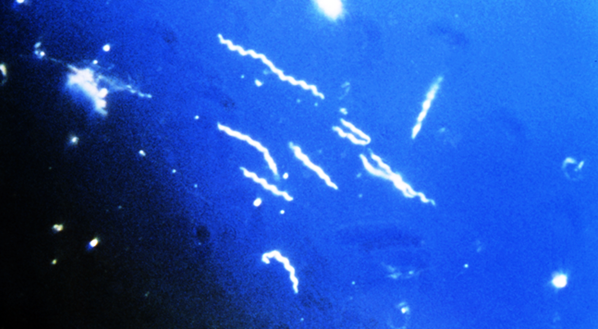
Now when it comes to Bb infections, the most important recommendation I have is to be really aggressive. I use a pincers approach. By that, I mean if you just use antibiotics and don’t boost the immune system, you won’t see a complete cure. If you just strengthen the immune system, it’s almost never enough. I’ve never seen a serious case of Lyme get better without antibiotics, and I’ve tried. The important thing with Lyme is to recognize that the Lyme organism metamorphosizes. The Lyme organism starts off as a spirochete, a strong cell-wall organism, and it’s hard to see under a microscope. It’s long enough to be seen, but it’s very thin. So, in order to see it under a microscope, you almost need to use a darkfield or lightfield microscope.
When you treat it with antibiotics, you start off with an antibiotic that kills the cell wall. The organism will start to die, but it’s a slow-growing organism. Most organisms with which we get infected are like E-coli, streptococcus, staphylococcus, pneumococcus and gonococcus, and they’re fast-growing organisms. They divide every twenty minutes when they’re infecting, so you get three generations in an hour. They are very vulnerable to antibiotics. Lyme, on the other hand, divides every twenty hours. Therefore, it’s much harder to kill. Its metabolism is much slower and deliberate.
If you get chronic Lyme, you can understand that instead of taking ten days to treat it, it can take ten months or more due to its slow replication. When you combine that with the fact that it’s intracellular and it hides very well from the immune system, hides from antibiotics, and metamorphosizes from a cell-wall phase to an L form, which is a form that does not have a cell wall, it becomes much more difficult to treat. There are also the cyst form and the granular forms which are resistant to most treatment and can remain dormant for years.
There are antibiotics that attack the protoplasm rather than the cell wall. They don’t work as well on the cell-wall form, during early Lyme, but somewhere around three weeks of azithromycin or clarithromycin (antibiotics we like to use on Lyme), the cell-wall form will metamorphosize. At first you may notice that you’ll start feeling better, and after about three weeks, you may stop getting better. So, then you add Doxycycline, and you continue both of them because the forms keep shifting back and forth. At the same time, you may be ignoring Babesia, which you may have if you haven’t checked for that. Even if you have checked for that, there are false negatives.
That’s why a doctor has to use clinical judgment. So, I often add Plaquenil, Metronidazole or some other parasitic drug, which can hit Babesia. Babesia is like malaria; it’s a parasite. There are a lot of herbals and nutritional boosters for the immune system. There’s a whole program I use including CoQ10, D-Ribose, L-Carnitine and Carnisine, una de gato (cat’s claw), and Artemisia. I like colostrum and sometimes colloidal silver and oral chelating agents. So, there are a number of things you can use, and it sometimes taxes the imagination to be able to prioritize. I can think of three hundred things that I could do, but I have to prioritize each case and find the best thing for that person that is possible at that time.
Tina: That’s so wonderful that you have that individualized approach. From a patient’s perspective, it’s so important that, after seeing so many other doctors, to eventually find someone like you, Dr. Susser, who will work with a person. Perhaps you have already witnessed this in Lyme patients—that is, a bit of anxiety.
Dr. Susser: Oh, yes! I’ve had patients who just burst into tears because someone finally believed them!
Tina: Do you have any suggestions for other medical practitioners?
Dr. Susser: Be open to the possibility. One thing about Lyme is to never get cocky about it. Don’t ever get overly confident that you’ve reached a cure just because somebody starts feeling better for a while. I’ve seen a lot of relapses when people quit too soon. That has to do with this twenty-hour replication rate and also with the idea that Lyme is intracellular and hides from the immune system. Remember that it can go into a cyst or granular form. It can become dormant. There are a lot of other diseases that are like that. Tuberculosis is like that.
Tina: Why won’t the medical community accept that Lyme is like tuberculosis in its ability to evade and lie dormant?
Dr. Susser: I don’t know. There is lots of evidence to show Lyme’s ability to lay dormant. Tuberculosis takes up to a year and a half to treat. When you first catch tuberculosis, it may only seem like a mild flu. It doesn’t necessarily cause a serious illness, and it leaves a little calcified nodule in the lung that has live tuberculosis organisms in it that are dormant.
When you get older, maybe 50 to 70 years old, you get pneumonia, cancer or some debilitating condition like alcoholism, the tubercle breaks down and you get tuberculosis. You then get a cavitation in your lung and a terrible disease, but it’s something you caught fifty years before. So, why would it be a surprise that other bugs can do something like that?
An astounding aside to this conversation is that about hundreds of millions of people worldwide are infected with dormant tuberculosis.
Tina: Have you observed an AIDS type syndrome develop from Lyme disease infection?
Dr. Susser: I haven’t yet seen anyone with Lyme as bad as terminal AIDS. I’ve seen some people who are pretty sick, but not with AIDS. AIDS is really dreadful. I used to see a lot of AIDS before the protease inhibitors were made available. These drugs suppress some of the action of the virus and they sure have prolonged a lot of lives and improved quality of life. I hardly see AIDS patients anymore.
There are some people that say that HIV has nothing to do with AIDS, and I don’t believe that for a second. I think there’s a very strong correlation from everything I’ve seen. I haven’t seen anyone with AIDS that didn’t have a positive HIV. Everyone with HIV starts getting the immune system changes and if you do a T-cell subset, you see a lowering of the helper cells and an increase of the suppressor cells. When the ratio gets very low, the infections get very bad.
I saw one young man die very quickly when he got pneumonia. He needed to be hospitalized, so I sent him to UCLA, but he didn’t get there in time. They started treating him, but he died very quickly. Every patient I’ve seen who had lethal AIDS had a positive HIV. Then I started seeing the ones with lethal AIDS start turning around with protease inhibitors, but most of them go to infectious disease doctors who specialize in protease inhibitors
Tina: What is your take on the political aspect of Lyme disease?
Dr. Susser: Be politically active. I don’t know who’s politically active in fighting people like the IDSA. They’re very powerful, but ultimately, everything winds up political. I have a saying. “If you tell the truth and keep telling it, eventually, your word becomes the law of the universe.”
When it comes to health, be proactive. The more proactive a patient is with their health, the better they do, in my experience. People often come to me quite sheepish and apologetic. They say, “I looked this up on the Internet and I don’t want to tell you how to be a doctor and I don’t want to pretend I’m a doctor and such.” This is all nonsense. Patients don’t have to be apologetic for learning. Information is information and knowledge is knowledge. The important thing is to find somebody who can help you use that knowledge, because nobody is going to get enough knowledge to deal with it themselves.
For example, I could go to a lumber yard and buy everything I need to build a house. If I built that house, I don’t think anybody would want to step in it. I’m not going to be the one to build a house that you could live in or even survive in for a moment. But people learn enough to buy vitamins and sometimes drugs and do a lot of things for themselves, but they can also damage themselves that way.
I have people who bring me lots of good information and I use it. I remember reading about Sir William Osler; he was the modern Hippocrates, the idol of medicine around the turn of the last century. He was a brilliant clinician and people really listened to him and followed his teachings. He had a lot of sayings like Hippocrates. One of the things that he said that always stuck in my mind was, “Listen to the patient. He will tell you what’s wrong with him.”
So, I consider that one of the most important things I ever learned in medicine. It’s one thing to hear the words and another thing to hear the meaning. I’m very careful to listen to the meaning and to hear everything the patient says. A lot of doctors will just jump from the superficial finding to this, this and this and seven minutes later they’re done. You can’t do Lyme in seven minutes. I can treat an earache in seven minutes and tonsillitis in seven minutes, but that’s not really treating the whole situation. Sometimes you need to set up the immune system and nutritional system and find out whether it’s the first tonsillitis they’ve ever had. I can run people through and do an augensblick diagnosis—that’s German for blink.
I can do that, but it’s not very satisfying and it’s not very safe. You can miss some really important things if you don’t take a little more time and dig a little deeper. If people are frustrated and have a hunch that their doctor isn’t looking deeply enough or hearing them well enough, change doctors. Also change doctors if a doctor doesn’t want you to have another opinion. If you’re not getting well and your doctor doesn’t want you to have another opinion, then you need another opinion. At least that’s my feeling.
[Continue to part 2 of this interview]
I feel greatly blessed through acquiring such cherished friendships in my association with the Lyme community. Dr. Susser has exhibited thoughtful medical care, compassion, generosity and friendship, and it was most memorable for me to peer through his panoramic window of medical experience during this interview. May I present the delightfully comical and impressive, Dr. Murray Susser.
Tina: So, Dr. Susser, it is also said that the journey of a thousand miles begins with the first step. With regard to your journey through medicine, would you please tell us what that first step was for you?
Dr. Susser: Yes. I graduated from the University of Pittsburgh Medical School in 1966. I went into family practice and very quickly, within the first year, I realized that medicine didn’t work the way I wanted it to. In other words, it wasn’t to my satisfaction. I started looking for alternative solutions, because people weren’t getting better. I tried a lot of different things, and finally, I stumbled onto Vitamin E. A friend of mine kept bugging me to read a book called Vitamin E for Ailing and Healthy Hearts by Wilfrid E. Shute, M.D. At the time I told my friend, “This is a quack book, but I’ll read it if you promise to never ask me about vitamins again.”
So, I read the book and Shute talked about treating 30,000 people with Vitamin E and all the great results he had with scar tissue, heart disease, high blood pressure, venous disease and blood clots, impotency and sexual dysfunction and all sorts of various disorders. At first I thought this guy must have been confabulating or was Baron von Munchausen.
Around that time, a patient came to see me who had suffered with venous disease of her legs for thirty years and had seen many doctors. She had terrible varicose veins that would develop infection and swelling andphlegmasia alba dolans. Phlegmasia means swelling, alba means whitish and dolans means pain. So, she had white, swollen, painful legs. If you just touched them with your finger, she would scream. There is a test, the Richardson test, where you wrap a blood pressure cuff around the leg and inflate the cuff, and note when it becomes painful. Well, when I put the cuff around her leg, she screamed, so I couldn’t even puff it up.
So, I asked her about all the ordinary things that could be used and she had used all of them and none of them had worked. Then I remembered Wilfrid Shute had said Vitamin E 800 units a day. So, I sent her to the drug store to get 800 units a day of Vitamin E, and she started doing that. When she came back in three weeks, she was almost cured! I was stunned! When I put the blood pressure cuff around her leg, I ran it up to the top, 300 milliliters of mercury and there was no pain. I was really excited and thought, “This cannot be a coincidence; this is a miracle.” The funny thing is, the woman wasn’t the least bit surprised and almost not appreciative. She just thought I was doing my job by getting her better.
I followed her for a couple months more and she was virtually cured with 800 units of Vitamin E a day. At the time, 800 units scared me, because I thought it was a high dose. I now sometimes put people on 20,000 units and I’ve had good results doing that. And I have a patient now who has been getting an epidural injection for spinal pain every two months for years. I started her on 10,000 units of Vitamin E a day and she’s worked up to 17,000 units, but she’s now gone eleven months without an epidural.
Now Vitamin E doesn’t work too well on nerve pain, but does work on bruises, soft tissue pain, sunburn and spider and insect bites very well. It also works for post-accident, soft-tissue injuries. So, they called me the “Vitamin E King” because I’ve used so much Vitamin E.
And all this business about Vitamin E being dangerous was the biggest propaganda of all time. It was based on a meta analysis, which is a study in which you take a bunch of lousy studies, put them together in a statistical manner and statistically maneuver it, to show that you compare some parameter with the treatment you’re interested in. So, I think the way they did it was with twenty-some studies comparing patient death with the amount of Vitamin E they took. That wasn’t only what the study was about; that was the data in the study. They took the seven studies with the highest death rates and found out how much Vitamin E these people were using and they found that these people were using more Vitamin E than the other studies. So, they said that high Vitamin E was related to high death rate. Then they published that study as if it were factual, but it was skewed. You know what Mark Twain said about statistics--that there are three kinds of lies—there are lies, damn lies and there are statistics.
It’s just like the Bible; the Devil can quote scripture to suit his purpose. So, anyhow, I got into Vitamin E and that opened the door for me. Then I started to look for more and more alternatives. And I was very excited. On my regular hospital rounds, I went into the doctors’ dining room where I went every day for lunch. I said, “Hey! Look what I found!” And all the doctors told me it was nonsense. They said, “Oh, Susser, you’re crazy! It was just coincidence!” But it wasn’t coincidence; it was way, way out of the realm of coincidence. They couldn’t believe that Vitamin E could be that powerful.
I saw it happen, so I knew it was true. That started me on my odyssey in nutrition. I saw a lot of surprising things happen. I had one guy who was scheduled to have a heart transplant, in the early days of heart transplants, when patients would live for a week afterwards at most. He got mad and walked out of the hospital, because he was waiting for a donor. He came to see me and said, “I don’t have long to live. Put me on something, some Valium maybe.” I asked him if he wanted to try some Vitamin E. He said, “What’ve I got to lose?”
So I put him on Vitamin E, and a year later he was playing golf and carrying his clubs without a cart! He never had a heart transplant, never had heart surgery, and he was fine for a long, long time. Then shortly after that, he called with an emergency saying he had stomach pain. It was the day after Thanksgiving and he said he ate too much turkey. I thought it may have been his heart, so I put him in coronary care. He insisted that it was his stomach, but I didn’t want to take any chances with him.
So I had Brian Kennedy, my cardiology friend, see him. Kennedy said, “This is an amazing case. This guy was supposed to have a heart transplant. He should have been dead a long time ago.” I said, “Well, Brian, what do you think of vitamin E?” And he walked away. And he was a good friend. But he couldn’t see the possibility that Vitamin E could have done this.
Tina: It’s really hard for some doctors to “cross over” isn’t it?
Dr. Susser: Well, it wasn’t too hard for me. A lot of doctors see it and they don’t believe it. They’re afraid to think outside the box. Remember, I was a jet fighter pilot -- now we’re talking fear.
Tina: Is it something one picks up in medical school that causes this denial?
Dr. Susser: But seriously, I think it has to do with the way we’re brought up. I had a lonely upbringing. My father was estranged and had a bad accident when I was younger and my mother was busy working and taking care of the family. She was too busy to pay much attention to me. I was the youngest of five. Nobody paid much attention to me, and I had to grow up on my own. I didn’t have a lot of dogma telling me how to live in the world. So, I had to learn everything myself. I had a good brain, I always made good grades, I had a good memory and I could learn quickly.
I grew up in a very smart family, everyone was very smart. So, I did things in my own way. It’s not a big leap of faith for me to see something that’s not in the conventional box. So, what I wound up doing, which was really most interesting and satisfying to me, was to treat people who slipped through the cracks of conventional medicine.
First I learned about Vitamin E and then I read Linus Pauling on Vitamin C. I saw the miracles with Vitamin C, too. I read Adele Davis who was a great nutritional guru who wrote some great books around that time. I got her on the phone and she was excited to hear from an M.D. who was interested in nutritional medicine. I went to a convention in San Francisco , where I met her, and she became my mentor. I started using vitamins according to what she wrote in her books and I learned about other nutritionists around the country, such as Carlton Fredericks, whom I could call.
These great nutritionists were all marginalized by conventional medicine. They were all considered quacks and attacked in various ways by the media. I kept a low profile and just did my nutritional stuff, and then I went to a meeting and learned abut hypoglycemia from Harold Harper and Carlton Fredericks. Conventional docs thought that hypoglycemia was another non-disease, a notion. Hypoglycemia is very real.
Tina: Was there testing for it at the time?
It was hard to test; it was a clinical diagnosis. You can do a glucose tolerance test and find hypoglycemia, but it’s a miserable test. The conventional docs wouldn’t agree to it, though. Hypoglycemia was defined as having blood sugar below 40, but your average blood sugar was 65 to 115. Now they’ve made it 65 to 99, which means that the American Diabetic Association can get more people called diabetic. They keep lowering the levels. For instance, blood pressure of 140 was considered borderline. Now, 120 over 80 is considered normal and 121 is now considered pre-hypertensive, so they can give hypertensive drugs much sooner.
Anyhow, I started learning about hypoglycemia. The normal hypoglycemic level of 65 is way too low; the normal should not be less than 90 or 85. They call 65 the low normal and they call 40 hypoglycemia. So, what is it if it’s between 40 and 65? I was at an affair at the medical school and I saw Dr. Fielding, who was our Chief Endocrinologist and my endocrinology professor while I was in medical school. So, I said, “Dr. Fielding, I have a question about blood sugars. If 65 is the low normal and 40 is hypoglycemia, what is 50?” And he answered, “Borderline.” You mean that whole realm from 40 to 65 is borderline and 70 is normal?
So, it was considered a non-disease and never treated. In fact, the New England Journal of Medicine published an editorial on the epidemic of a non-disease called hypoglycemia. It’s really a form of malnutrition and has to do with all sorts of problems including depression, anxiety, confusion--and obesity is very much related to hypoglycemia. So I went from disease to disease just like that. Then I learned about chelation and treated vascular disease with intravenous chelation and became experienced and successful doing that. This helped a lot of people and I had a lot of success with patients using chelation.
Tina: I had a primary care physician once who refused to consult with my Lyme doc, because my Lyme doc used chelation. The PCP surprised me by telling me that he signed a promise or statement when he finished medical school that he would never use chelation. I thought that was outrageous.
Dr. Susser: Chelation wasn’t that popular when I graduated, but that’s almost violating something in the Constitution. I think that’s an unconstitutional thing to do. I can’t imagine a medical school would do that.
Chelation means metal-binding. It was originally used, and is still used, for heavy metal poisoning. However, in conventional medical wisdom, chelation is only used for heavy duty metal poisonings. That would mean a lethal amount from a laboratory or an industrial accident, or if a child gets into a bucket of paint or eats paint chips, or someone swallows mercury. The chelators used would be EDTA or BAL, which is a mercury chelating agent.
These chelators bind lead, cadmium, mercury, tin, silver and nickel. The most toxic metals we deal with are mercury, lead and cadmium. It’s interesting that mercury wasn’t even discovered as a toxin until about twenty years ago. When I used to do hair analysis and I’d find high mercury, I would wonder what that would mean. No one seemed to know. Then Hal Huggins did some important work with mercury in his dentistry practice in Colorado , and he came up with some of the first discoveries of low-level mercury as a poison.
The poisonous level we’re talking about is several orders of magnitude below the laboratory and industrial poisoning. It’s a low-grade, insidious poisoning that poisons our arteries, our brains and our endocrine and immune systems.
Tina: Which is really important in our day and age, right? Aren’t we being bombarded with these toxic metals?
Dr. Susser: Well, improvements have been made, such as removing lead from paint, gasoline, solder and pipes. We used to have a lot of exposure to lead, but we’ve decreased it enormously. It is still too much, though. Mercury has been a major problem, but they’re decreasing that. Except now all the new light bulbs will have mercury in them and that’s going to cause a mess. There is still lead in some of our water pipes, and there are other industrial sources as well. Breathing gasoline fumes and getting gasoline on your skin can cause exposure to lead, also.
A big source of mercury is fish like tuna and swordfish, which are heavily loaded with it. Silver amalgam fillings in teeth are fifty percent mercury and we’re getting a lot of mercury from those. Many dentists are stopping this practice, but the American Dental Association has managed to keep them legal and is still saying that silver-mercury amalgams are a valid thing to do. There are some countries now which are banning these amalgams, especially in pregnant women and children. I think Sweden , Finland , Germanyand other parts of the world are starting to ban mercury fillings in certain populations, but there is a lot of legality involved in all of that.
Mercury also comes from the fumes of power plants that burn coal and other fossil fuels. So, if you’re near a power plant that’s spewing out smoke, it’s probably pretty polluted. There are silver-mercury batteries and mercury switches in our walls and lights. We’ve gotten rid of mercury thermometers, so that helps. The heavy metal picture is probably, overall, getting better. However, chelation is something that can be a real deterrent to accumulating these metals.
Tina: I’ve heard that chelation works on plaque in arteries.
Dr. Susser: As a doctor who uses chelation, I legally can’t say that chelation works on arteries. I can tell you that my experience is that chelation takes cadmium and lead out of the arterial wall, and cadmium and lead, and mercury to some extent, are known to block the action of nitric oxide. Nitric oxide opens arteries and is blocked by these heavy metals. Therefore, logically, you would think that by blocking the nitric oxide, your arteries would tend to clamp down, spasm, close up and cause damage. Nitric oxide is a natural substance in our bodies that is made in large part from arginine, which is an amino acid. So, taking amino acids is a good way to open up your arteries. We’ve found that arginine is very helpful in high blood pressure, because high blood pressure will result from lack of nitric oxide.
Chelation is really wonderful in many ways. It cleans out these toxic elements in your body. It may be hard not to eat tuna fish, swordfish, halibut, king mackerel and even orange roughy is pretty high in mercury. This is interesting; you know, the safest fish you can eat is wild salmon, because it has beautiful oils and it has almost no mercury because it eats krill. Krill does not accumulate mercury. Whereas, farm salmon eat small fish and small fish have mercury in them. The more fish they eat, the more mercury they accumulate. This is called biomagnification. So, farm salmon biomagnify the mercury like any other big fish.
If you don’t study it, it’s hard to know what’s safe to eat. I still love tuna sushi and I know when I’m eating the mercury it’s not good for me, but I take a lot of oral chelators, such as EDTA and DMSA. Now, oral is not as good as intravenous chelation, because all the oral chelators have to go through the liver where they use up most of their chelation by taking toxic metals out of the liver. That’s very good for you, but it doesn’t help the muscles or your other organs very much. If you take the oral chelation long enough, maybe years or decades, and get your liver completely cleaned out, then you start getting the other parts of your body. These heavy metals have a long half-life in the body. Lead, cadmium and mercury probably have a half-life of between twenty and twenty-five years. That means that, if you have twice as much lead in your body as you’re supposed to have and if you don’t do anything to get rid of it, it will take your body twenty years or more to get it down to the ideal level. That is, so long as you don’t add any more.
Tina: How do you integrate all this knowledge in your approach to patients?
Dr. Susser: My current practice is using all the elements that I’ve used over the years and I’ve found that the disease that is the most damaging, the most prevalent that slips through the cracks of conventional medicine the most, is Lyme disease. Lyme disease is rampant in the east and it is becoming more and more prevalent in the west. It was discovered in Lyme , Connecticut ; that’s where the name came from, where they first described the disease in this country. It’s a tick-borne disease--that’s what it’s famous for.
These are Ixodes ticks which bite this certain kind of deer that are common on the east coast. These deer are often infected with Lyme and other bacteria that can be carried by ticks. So, there’s Lyme and the co-infections. The co-infections are Babesiosis, Erlichiosis, Bartonella, Brucellosis, mycobacteria, and of course, ticks carry the rickettsial diseases like Rocky Mountain Spotted Fever. So, there are a lot of things you can get from a tick bite, and some ticks will carry two and three different bugs when they bite you. They used to say that one tick out of a hundred would carry Lyme, but now they’re saying one tick out of two will carry the disease.
If you get a tick bite, there’s a high likelihood of getting Lyme disease. If you do get a tick bite, get the head of the tick out with a little pair of pliers. Some people say you can cook it out of there, but that doesn’t work. A good thing to do is to save the tick, freeze it or put it in formaldehyde and have it tested. In the meantime, I would take antibiotics for three to four weeks and maybe longer, just in case, because the likelihood of infection is too high.
Tina: This protocol is entirely different than the Infectious Diseases Society of America treatment guidelines, which recommend only 200 mg of Doxycycline with the fulfillment of some absolutely ludicrous attachment and endemic criteria. I would take your treatment over theirs any day.
Dr. Susser: Yes, they’re really out of touch, really out of touch. The Infectious Diseases Society of America has been accused of having conflicts of interest. The IDSA panel made the announcement that chronic Lyme disease doesn’t really exist, and it turns out they probably had financial interests with insurance companies. The Attorney General of Connecticut brought charges against them.
My approach to patients is one of partnership in helping with their diseases. I am the junior partner; the patient is in charge. I will be the best advisor I can possibly be. I will offer options, because most of the things that I do don’t have rigid protocols. Like the old days--strep throat, ten days of penicillin or pyelonephritis, seven days of Keflex. There are a lot of rigid protocols in medicine and most of the things I work with are conditions like chronic fatigue syndrome, which is one that falls through the cracks. It was mostly considered to be an emotional disorder or depression. I’d say that if you had your life taken away by an illness, wouldn’t you be depressed?
So, this book I wrote twenty years ago on Chronic Fatigue Syndrome is still valid in many ways, because the principles contained within it are what I apply to my patient approach. I look at all the possibilities and offer what certainty I can to patients. One of my strengths in medicine is that I’m willing to live with uncertainty and most doctors are not.
For example, one thing that I know is that something caused your disease, but I don’t know what it is. It has to be in some category or another—a bacteria or a toxin or allergy. So, I take the most likely possibility and design a good safe therapeutic trial and do that. Now, with Lyme, the testing has recently given us much more certainty, with Igenex Lab and tests like the CD57. There are a number of things that give us much more information about Lyme.
So, I had a patient just today who had her tick bite twenty-some years ago, with a bull’s eye rash and everything, and she’s probably been to fifteen doctors, none of whom would believe she has Lyme. She has Lyme tests from labs that don’t do well with Lyme and they came back equivocal or negative, so she didn’t have Lyme by any standard for all these years. Yet, she has all the classic signs of Lyme—myalgia, arthralgia, brain fog, classical rash in New York , and her mother recognized it. She has Lyme clinically. In two weeks, if the testing comes back positive, there’s a ninety-six percent chance she has Lyme. I say that, just from her clinical history, there is a ninety-nine percent chance she has Lyme, no matter what the test shows. She’s been sick all these years.
I even use the principals of Thomas McPherson Brown, who was the great rheumatologist at George Washington University Medical School . He discovered that he could cure sixty percent of his rheumatoid arthritis patients by giving them minocycline, an antibiotic, for ten months. He found Chlamydia in the joints of rheumatoid arthritis patients, which is a bacterium. He didn’t know anything about nutrition or probiotics and he was a major player in conventional medicine. He published in peer reviewed journals, and not only that, he was in Washington , D.C. and was the rheumatologist for three different presidents in White House. This guy was big time and he was ignored by conventional medicine. It’s one thing if they ignore me here in my little office, but to ignore Thomas McPherson Brown is really insane. I now have seen many patients who came to me with a diagnosis of rheumatoid arthritis; I discovered Lyme and treated them successfully – no more rheumatoid arthritis!
Tina: Have you ever treated a patient who presented with a bull’s eye rash?
Dr. Susser: Yes, and I treated the patient for three weeks, and they never got Lyme. And, of course, the earlier the diagnosis, the easier it is to treat.
Tina: Are you finding Lyme cases here in Arizona ?
Dr. Susser: I treat patients who acquired Lyme in other states, and I have patients who travel from northernCalifornia , Utah , New Mexico and Florida . As for Arizona , absolutely, quite a few. Most of them have been around for a long time, months or even years. I’ve seen acute cases, but curiously enough, not with a tick bite. There are other insects that might carry it, maybe fleas, mites, mosquitoes or houseflies. There are definitely more mammals than deer who carry it, like mice and squirrels and rabbits. And I know horses and dogs can get it, too. So, there are many animals that carry Lyme and it’s getting more and more prevalent. At the same time, we don’t have any really good answers for it. The antibiotics are a poor answer for it, but at least if you catch it early, it can work very well.
CFS is another disease that slips through the cracks. It was first named by Paul Cheney and Dan Peterson in Incline Village , Nevada . They had a flu epidemic and some of the people remained sick. That was the time when the Epstein Barr test first became available on the clinical market. All these people began testing positive for Epstein Barr and they decided it was an Epstein Barr epidemic, which it turned out not to be. It turns out that Epstein Barr, which is Human Herpes Virus 4, is in all of us and when you get a serious illness, the HHV4 virus flares.
That led to confusion between Epstein Barr and CFS. When they found out that CFS was not caused by EBV, they decided it was an emotional disease and a form of depression. It was a crippling disease and in some cases it probably was Lyme. The definition of CFS is fifty percent debility for greater than six months with no known cause. It also has other symptoms like muscle pain, joint pain and swollen glands. So, myalgia was a common accompaniment.
In my book that I wrote with Michael Rosenbaum, called Solving the Puzzle of Chronic Fatigue Syndrome, I came up with the idea prior to that of Mixed Infection Syndrome. Again, the wisdom of conventional medicine is that you can only have one infection at a time until you’re dying, and then you can have all these opportunistic infections that take hold. In my opinion, “opportunistic” is a redundant word, because all infections are opportunistic. They look for the opportunity to invade. What they mean is that an infection needs a real strong opportunity.
We are constant besieged with bacteria and various organisms in the body. There are five hundred different bacteria that live in the gut. There are hundreds that live in the mouth, live under our fingernails and live on the skin. So, we have many different bacteria. The total count in the gut is variable. Some people say it’s three trillion and some people say it’s much more than that. How do you count them; it’s hard.
The point is that in CFS as a diagnosis, it will disappear when we are smart enough to diagnose all the different infections and all the different toxicities that can cause chronic fatigue. Lyme is a perfect example. Lots of these people we’ve labeled with CFS have Lyme disease. When we discover the Lyme disease, it’s no longer CFS; it’s chronic fatigue from Lyme disease. If they also have Babesia or some other co-infection, it’s Mixed Infection Syndrome. They commonly have been on antibiotics for one reason or another and get an overgrowth of yeast in the gut. Then they have some sort of fungal or yeast infection. Then that opens the door to parasites and to other forms of bacteria that can invade, such as clostridium dificile and things of that nature. So, there are a number of organisms that will invade under these circumstances, and the patient is not terminal. The immune system is not totally collapsed. It’s just collapsed enough. Then there are confounding factors like toxic metals and toxic fungus and molds in the house. One good thing about Lyme and the co-infections is that they validate my theory from twenty years ago that we get mixed infections.
A leaky roof or a leaky water pipe will lead to black mold, one of which is Stachybotrys. Stachybotrys toxins can be crippling and can lead to chronic fatigue and immune system depletion. Then the yeast, bacteria and parasites can invade. So, I would consider all these things in a patient with CFS symptoms, but not necessarily test for all of them. When you start testing for all these things, you run out of blood and money pretty quick. If I tested for all the things that are possible, I could drain somebody’s bank accountand their whole vascular system. Therefore, I use my best clinical judgment, and I have a lot of experience doing that.
Tina: What would you say is the difference between Chronic Fatigue and Fibromyalgia?
Dr. Susser: Aside from the fact that they commonly occur together, it is a case of which came first—the chicken or the egg—fibromyalgia means muscle pain and chronic fatigue is just that, chronic fatigue. You can have one without the other, but they commonly occur together. Fibromyalgia is fatiguing, and some people start off with fatigue and the fibromyalgia follows.
Now when it comes to Bb infections, the most important recommendation I have is to be really aggressive. I use a pincers approach. By that, I mean if you just use antibiotics and don’t boost the immune system, you won’t see a complete cure. If you just strengthen the immune system, it’s almost never enough. I’ve never seen a serious case of Lyme get better without antibiotics, and I’ve tried. The important thing with Lyme is to recognize that the Lyme organism metamorphosizes. The Lyme organism starts off as a spirochete, a strong cell-wall organism, and it’s hard to see under a microscope. It’s long enough to be seen, but it’s very thin. So, in order to see it under a microscope, you almost need to use a darkfield or lightfield microscope.
When you treat it with antibiotics, you start off with an antibiotic that kills the cell wall. The organism will start to die, but it’s a slow-growing organism. Most organisms with which we get infected are like E-coli, streptococcus, staphylococcus, pneumococcus and gonococcus, and they’re fast-growing organisms. They divide every twenty minutes when they’re infecting, so you get three generations in an hour. They are very vulnerable to antibiotics. Lyme, on the other hand, divides every twenty hours. Therefore, it’s much harder to kill. Its metabolism is much slower and deliberate.
If you get chronic Lyme, you can understand that instead of taking ten days to treat it, it can take ten months or more due to its slow replication. When you combine that with the fact that it’s intracellular and it hides very well from the immune system, hides from antibiotics, and metamorphosizes from a cell-wall phase to an L form, which is a form that does not have a cell wall, it becomes much more difficult to treat. There are also the cyst form and the granular forms which are resistant to most treatment and can remain dormant for years.
There are antibiotics that attack the protoplasm rather than the cell wall. They don’t work as well on the cell-wall form, during early Lyme, but somewhere around three weeks of azithromycin or clarithromycin (antibiotics we like to use on Lyme), the cell-wall form will metamorphosize. At first you may notice that you’ll start feeling better, and after about three weeks, you may stop getting better. So, then you add Doxycycline, and you continue both of them because the forms keep shifting back and forth. At the same time, you may be ignoring Babesia, which you may have if you haven’t checked for that. Even if you have checked for that, there are false negatives.
That’s why a doctor has to use clinical judgment. So, I often add Plaquenil, Metronidazole or some other parasitic drug, which can hit Babesia. Babesia is like malaria; it’s a parasite. There are a lot of herbals and nutritional boosters for the immune system. There’s a whole program I use including CoQ10, D-Ribose, L-Carnitine and Carnisine, una de gato (cat’s claw), and Artemisia. I like colostrum and sometimes colloidal silver and oral chelating agents. So, there are a number of things you can use, and it sometimes taxes the imagination to be able to prioritize. I can think of three hundred things that I could do, but I have to prioritize each case and find the best thing for that person that is possible at that time.
Tina: That’s so wonderful that you have that individualized approach. From a patient’s perspective, it’s so important that, after seeing so many other doctors, to eventually find someone like you, Dr. Susser, who will work with a person. Perhaps you have already witnessed this in Lyme patients—that is, a bit of anxiety.
Dr. Susser: Oh, yes! I’ve had patients who just burst into tears because someone finally believed them!
Tina: Do you have any suggestions for other medical practitioners?
Dr. Susser: Be open to the possibility. One thing about Lyme is to never get cocky about it. Don’t ever get overly confident that you’ve reached a cure just because somebody starts feeling better for a while. I’ve seen a lot of relapses when people quit too soon. That has to do with this twenty-hour replication rate and also with the idea that Lyme is intracellular and hides from the immune system. Remember that it can go into a cyst or granular form. It can become dormant. There are a lot of other diseases that are like that. Tuberculosis is like that.
Tina: Why won’t the medical community accept that Lyme is like tuberculosis in its ability to evade and lie dormant?
Dr. Susser: I don’t know. There is lots of evidence to show Lyme’s ability to lay dormant. Tuberculosis takes up to a year and a half to treat. When you first catch tuberculosis, it may only seem like a mild flu. It doesn’t necessarily cause a serious illness, and it leaves a little calcified nodule in the lung that has live tuberculosis organisms in it that are dormant.
When you get older, maybe 50 to 70 years old, you get pneumonia, cancer or some debilitating condition like alcoholism, the tubercle breaks down and you get tuberculosis. You then get a cavitation in your lung and a terrible disease, but it’s something you caught fifty years before. So, why would it be a surprise that other bugs can do something like that?
An astounding aside to this conversation is that about hundreds of millions of people worldwide are infected with dormant tuberculosis.
Tina: Have you observed an AIDS type syndrome develop from Lyme disease infection?
Dr. Susser: I haven’t yet seen anyone with Lyme as bad as terminal AIDS. I’ve seen some people who are pretty sick, but not with AIDS. AIDS is really dreadful. I used to see a lot of AIDS before the protease inhibitors were made available. These drugs suppress some of the action of the virus and they sure have prolonged a lot of lives and improved quality of life. I hardly see AIDS patients anymore.
There are some people that say that HIV has nothing to do with AIDS, and I don’t believe that for a second. I think there’s a very strong correlation from everything I’ve seen. I haven’t seen anyone with AIDS that didn’t have a positive HIV. Everyone with HIV starts getting the immune system changes and if you do a T-cell subset, you see a lowering of the helper cells and an increase of the suppressor cells. When the ratio gets very low, the infections get very bad.
I saw one young man die very quickly when he got pneumonia. He needed to be hospitalized, so I sent him to UCLA, but he didn’t get there in time. They started treating him, but he died very quickly. Every patient I’ve seen who had lethal AIDS had a positive HIV. Then I started seeing the ones with lethal AIDS start turning around with protease inhibitors, but most of them go to infectious disease doctors who specialize in protease inhibitors
Tina: What is your take on the political aspect of Lyme disease?
Dr. Susser: Be politically active. I don’t know who’s politically active in fighting people like the IDSA. They’re very powerful, but ultimately, everything winds up political. I have a saying. “If you tell the truth and keep telling it, eventually, your word becomes the law of the universe.”
When it comes to health, be proactive. The more proactive a patient is with their health, the better they do, in my experience. People often come to me quite sheepish and apologetic. They say, “I looked this up on the Internet and I don’t want to tell you how to be a doctor and I don’t want to pretend I’m a doctor and such.” This is all nonsense. Patients don’t have to be apologetic for learning. Information is information and knowledge is knowledge. The important thing is to find somebody who can help you use that knowledge, because nobody is going to get enough knowledge to deal with it themselves.
For example, I could go to a lumber yard and buy everything I need to build a house. If I built that house, I don’t think anybody would want to step in it. I’m not going to be the one to build a house that you could live in or even survive in for a moment. But people learn enough to buy vitamins and sometimes drugs and do a lot of things for themselves, but they can also damage themselves that way.
I have people who bring me lots of good information and I use it. I remember reading about Sir William Osler; he was the modern Hippocrates, the idol of medicine around the turn of the last century. He was a brilliant clinician and people really listened to him and followed his teachings. He had a lot of sayings like Hippocrates. One of the things that he said that always stuck in my mind was, “Listen to the patient. He will tell you what’s wrong with him.”
So, I consider that one of the most important things I ever learned in medicine. It’s one thing to hear the words and another thing to hear the meaning. I’m very careful to listen to the meaning and to hear everything the patient says. A lot of doctors will just jump from the superficial finding to this, this and this and seven minutes later they’re done. You can’t do Lyme in seven minutes. I can treat an earache in seven minutes and tonsillitis in seven minutes, but that’s not really treating the whole situation. Sometimes you need to set up the immune system and nutritional system and find out whether it’s the first tonsillitis they’ve ever had. I can run people through and do an augensblick diagnosis—that’s German for blink.
I can do that, but it’s not very satisfying and it’s not very safe. You can miss some really important things if you don’t take a little more time and dig a little deeper. If people are frustrated and have a hunch that their doctor isn’t looking deeply enough or hearing them well enough, change doctors. Also change doctors if a doctor doesn’t want you to have another opinion. If you’re not getting well and your doctor doesn’t want you to have another opinion, then you need another opinion. At least that’s my feeling.
[Continue to part 2 of this interview]
About the author

Murray Susser M.D. is on the cutting edge of traditional and alternative medicine. Contact Dr. Susser: http://MurraySusserMD.com/contact (to ask a question or to make an appointment)
http://Facebook.com/MurraySusserMD
http://Twitter.com/MurraySusserMD
http://Facebook.com/MurraySusserMD
http://Twitter.com/MurraySusserMD
About the author

Tina J. Garcia is a Lyme patient and Founder of Lyme Education Awareness Program, L.E.A.P. Arizona at www.leaparizona.com.
latest posts

tags
Cowden Protocol month 1

23andMe genetic Testing
Disclaimer: The information on this website is not a substitute for professional medical advice.
Always consult with your treating physician before altering any treatment protocol.
Always consult with your treating physician before altering any treatment protocol.
